
Growth and Development — MCQs

On this page
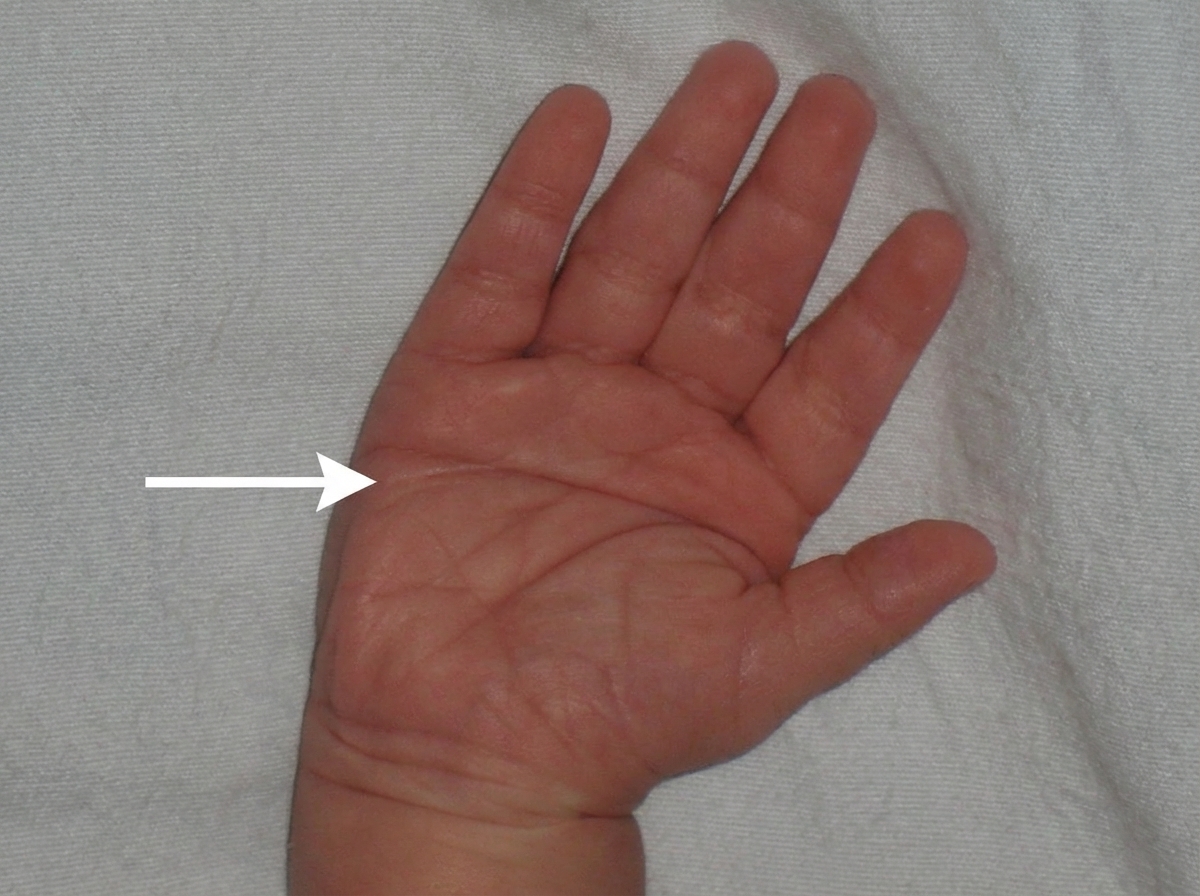
The image shows presence of:
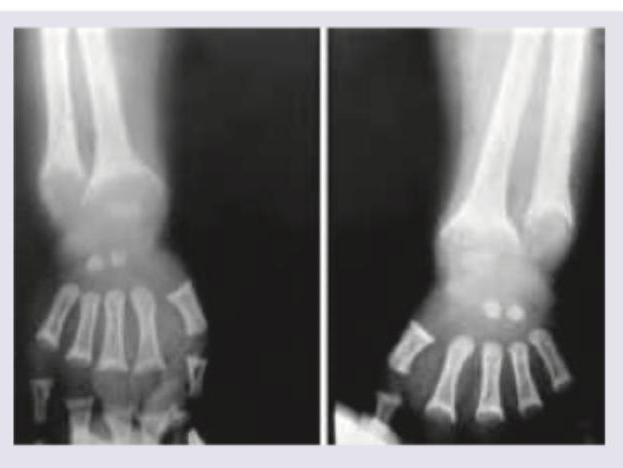
A 5-year-old boy from upper socioeconomic background presents with bowing of legs. On work up serum calcium was $9 \mathrm{mg} \%$ with serum phosphate of $1 \mathrm{mg} \%$ with normal serum alkaline phosphatase (ALP) and normal serum PTH. X-ray wrist joint is given. Comment on the diagnosis:
A child can perform this activity by what age?

The developmental milestone shown in the image corresponds to which age?

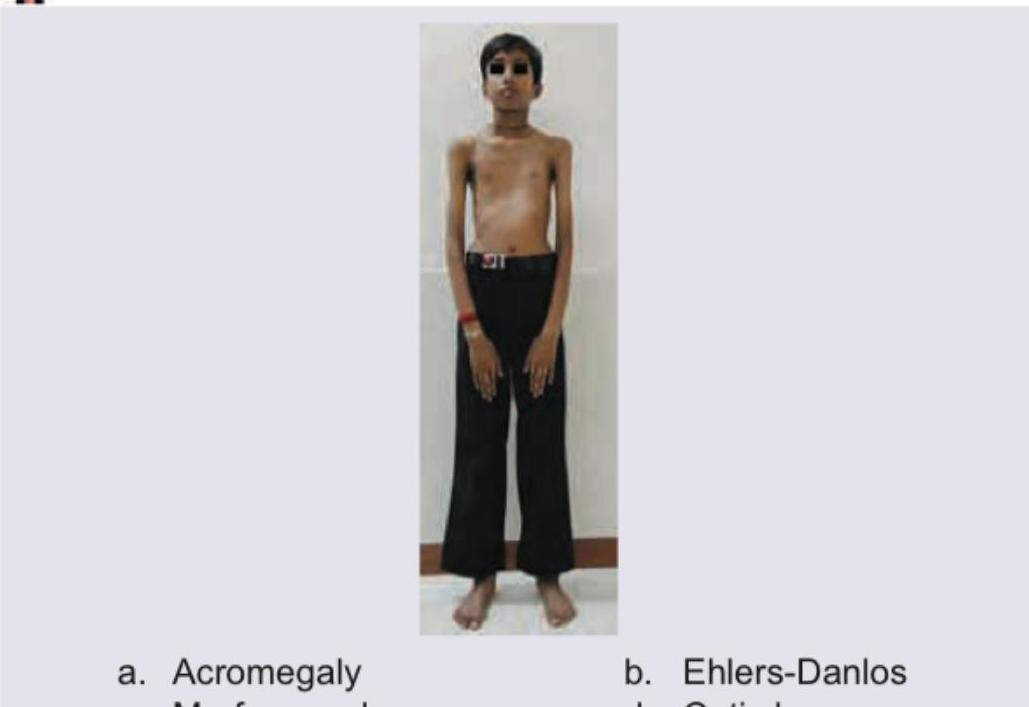
A 5-year-old short stature child is brought for evaluation. Which disease is the most likely diagnosis as depicted by these pictures of the child, foot and retina?

The image shows a child with:
The image shows a child with:

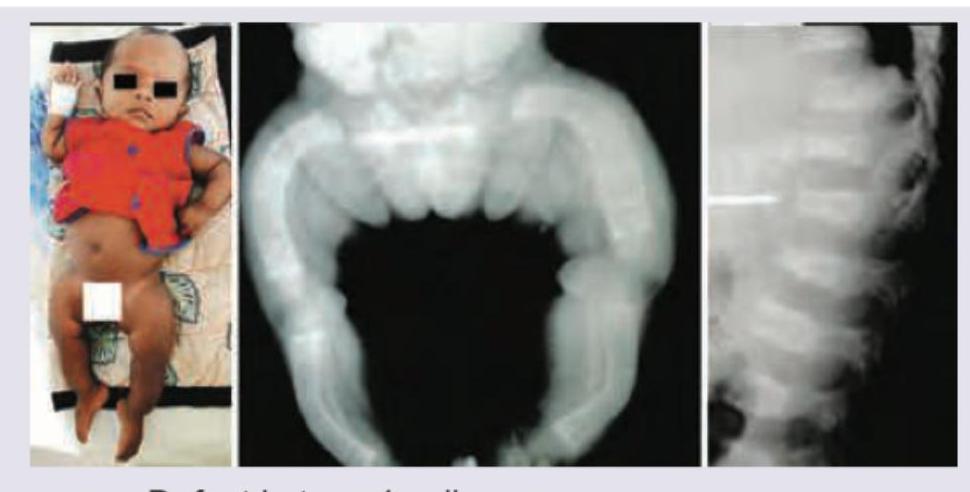
A 3-month-old infant with shortened bowed extremities, macrocephaly. X-ray of lower extremities and Lateral view spine was performed. All are true about the condition except: (Recent NEET Pattern 2016-17)
Which of the following is the probable diagnosis in this child with dwarfism, coarse facies. X-ray spine lateral view and X-ray hand is shown?

The following child has presented with disfigurement and rapidly progressive overgrowth of some body parts. The clinical diagnosis is?

Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app