
Growth and Development — MCQs

On this page
At what age does a child typically hug their parents?
What is the typical number of teeth present at 7 years of age?
Which of the following is NOT a characteristic of Rett syndrome?
What is the approximate percentage of HbF in a 6-month-old infant?
What is the earliest sign of male puberty?
Teeth that erupt within 30 days of birth are called:
Which of the following language milestones does NOT typically develop by 15 months of age?
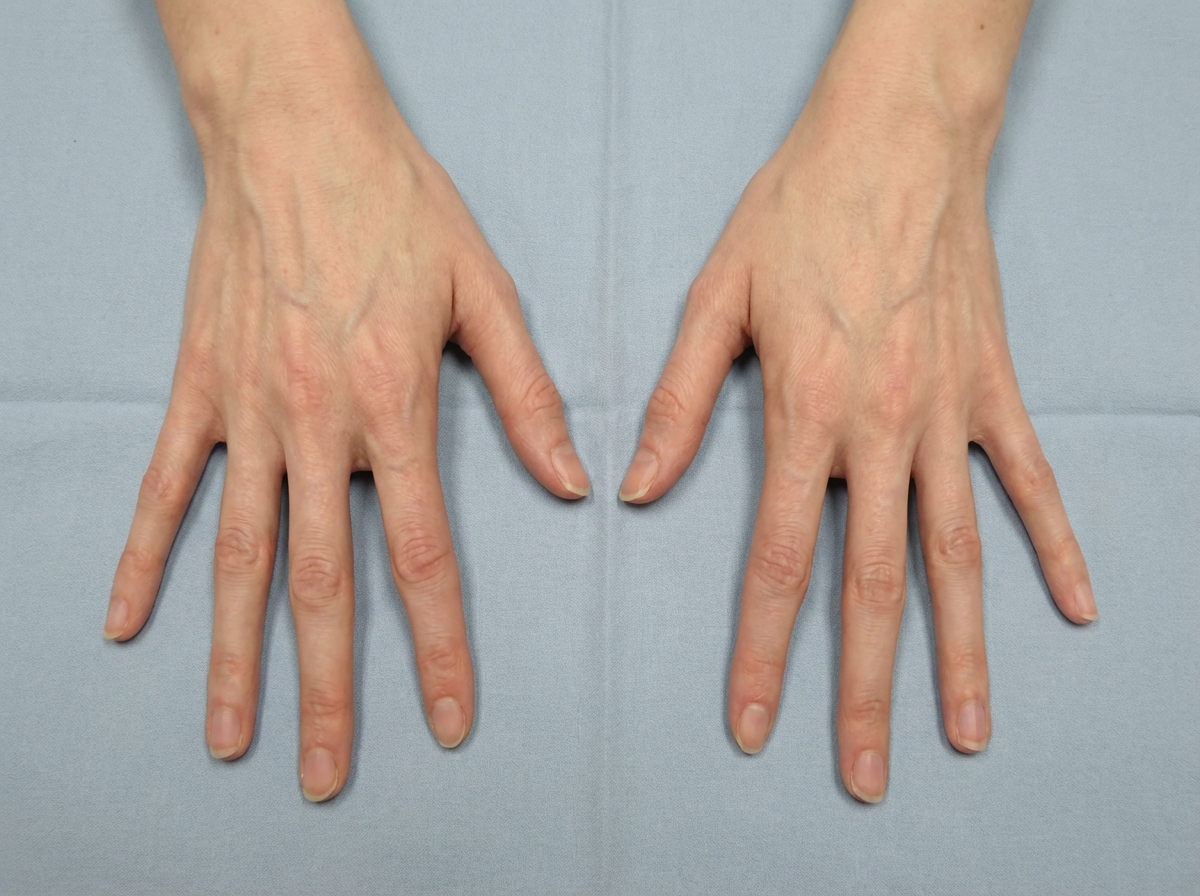
What is the disease in which these hand abnormalities are seen?
A child presents with failure to thrive. Despite counseling on nutritional improvement, the parents report no change. What is the likely diagnosis?
What is the approximate annual increase in height for a child before puberty?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app