
Growth and Development — MCQs

On this page
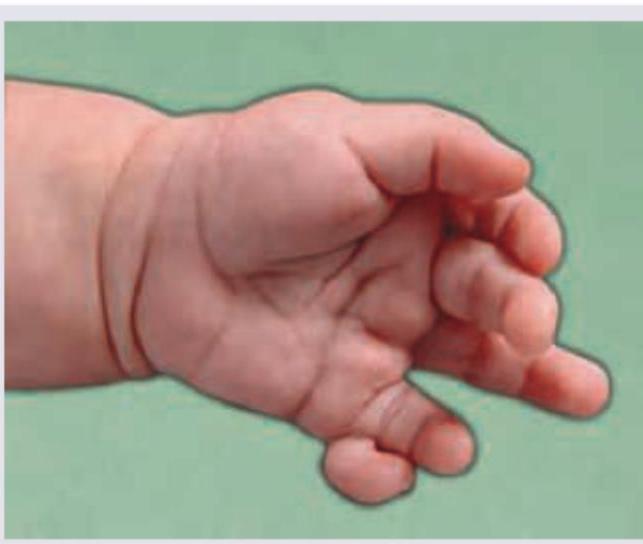
During evaluation of a child with obesity, following finding is observed. What is the association?
This baby has macrosomia along with organomegaly. Comment on the diagnosis from the hint given in the image?

Which of the following conditions is characterized by severe respiratory distress in newborns due to a small thorax, very short limbs, and a large head with midfacial hypoplasia and Cloverleaf skull deformity?
What is the dental condition shown in the image?

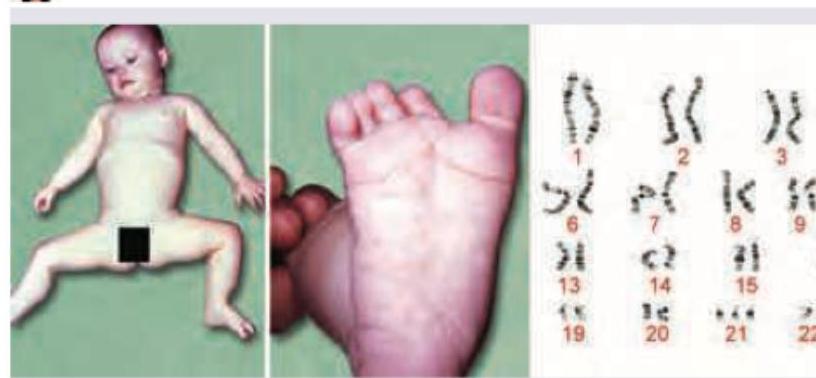
A newborn baby presents with hypotonia, flattened facial profile, and widely spaced first and second toes. The karyotype analysis is shown in the image. What is the most likely diagnosis?
A child can ride a tricycle, copies a circle, knows name and gender. The developmental age of this child is
A child can make a tower of 3 blocks, runs, copies his mother while sweeping and has a vocabulary of 8-10 words. His developmental age is
Child starts speaking short sentences by the age of :
Which of the following genetic disorders leads to intellectual disability?
Flattening of the growth curve in the growth chart signifies:
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app