
Growth and Development — MCQs

On this page
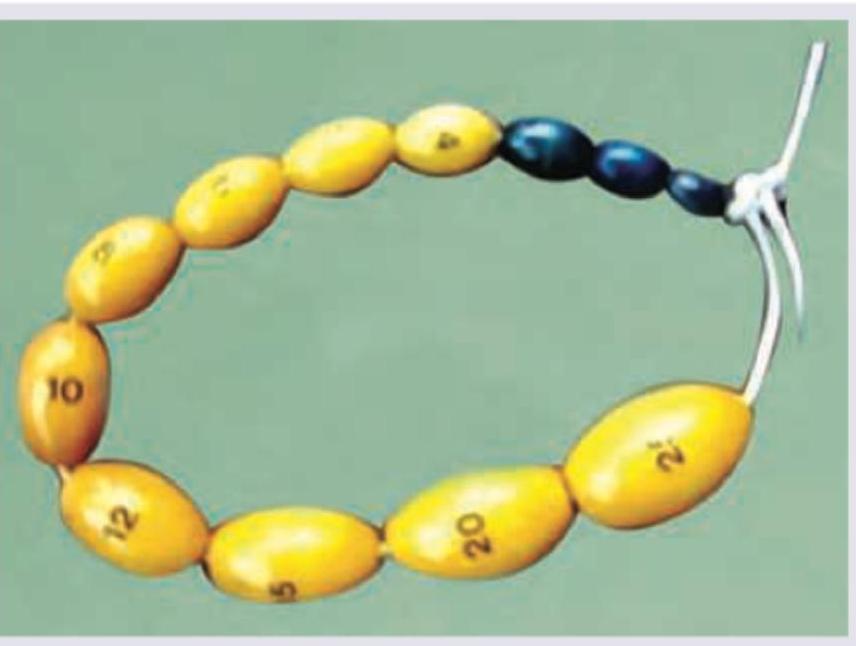
Which is true about the instrument shown?
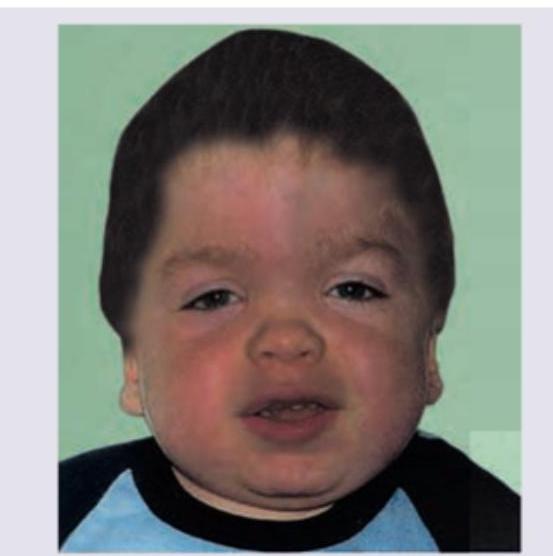
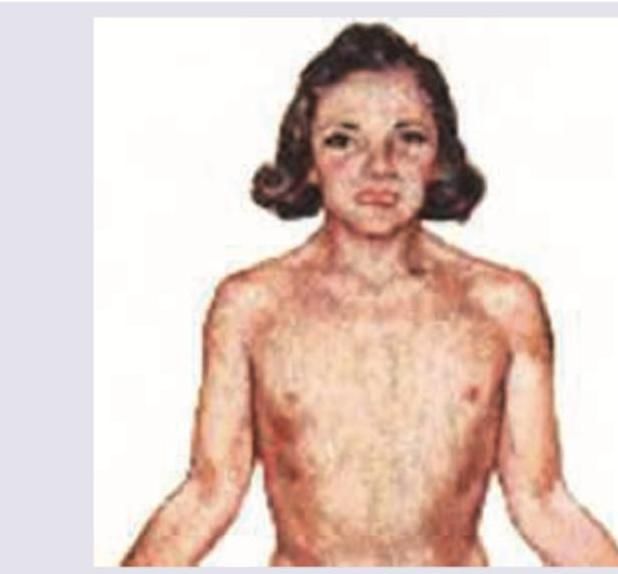
What is the diagnosis of this child with short stature and corneal opacity?
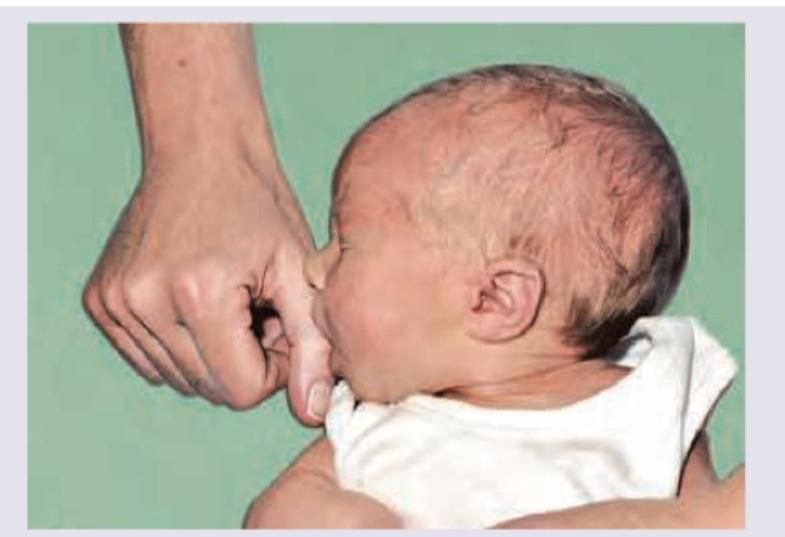
Which is true about the reflex shown in the image?
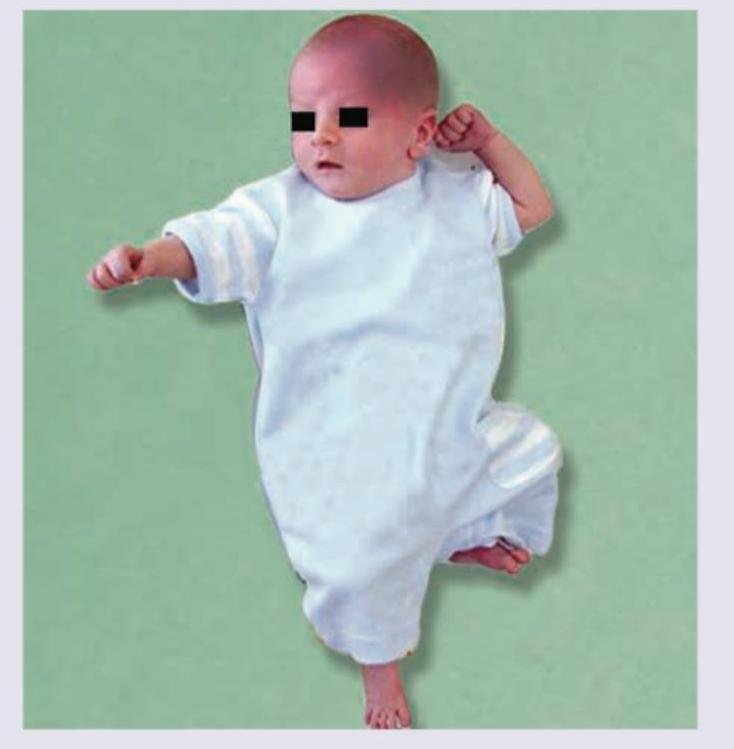
All are true about this reflex except:
The reflex shown below is normally integrated by what age range?
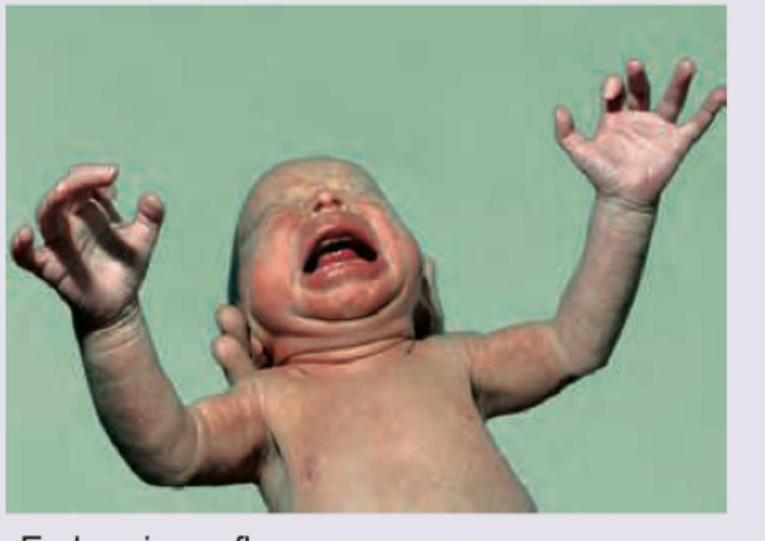
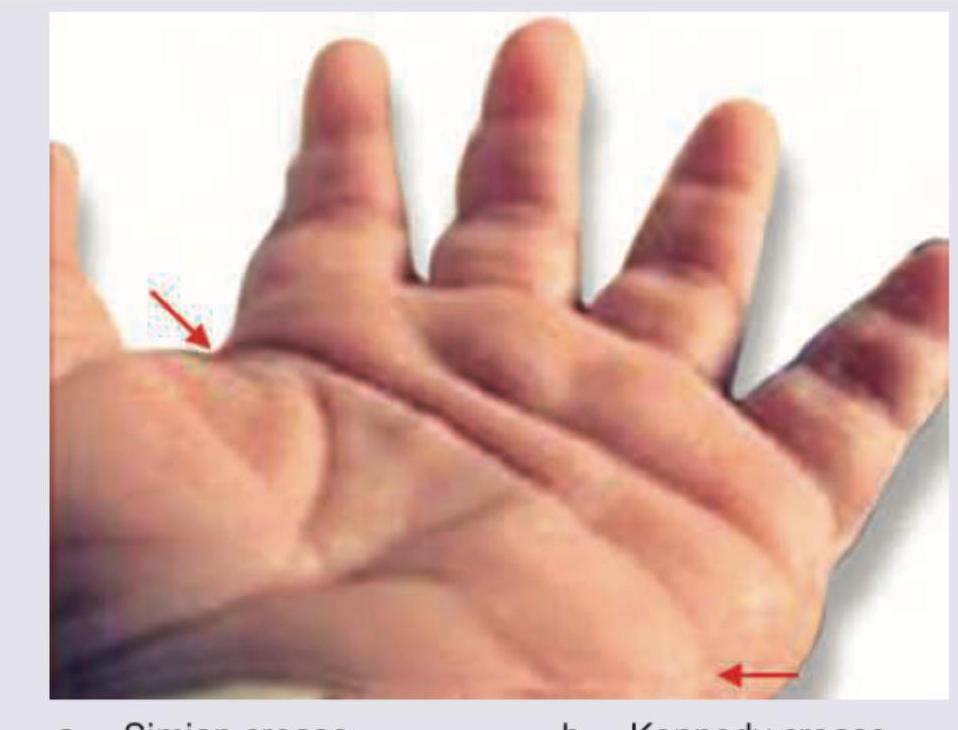
The image shows presence of:

A child suffering from respiratory and feeding difficulties was brought for consultation. All of the following are to be considered in differential diagnosis of the child except:
What is the expected karyotype in this phenotypically male child with the following findings and having pulmonic stenosis on Echocardiography?
During evaluation of a child with Down syndrome, the following finding is noted. Identify?
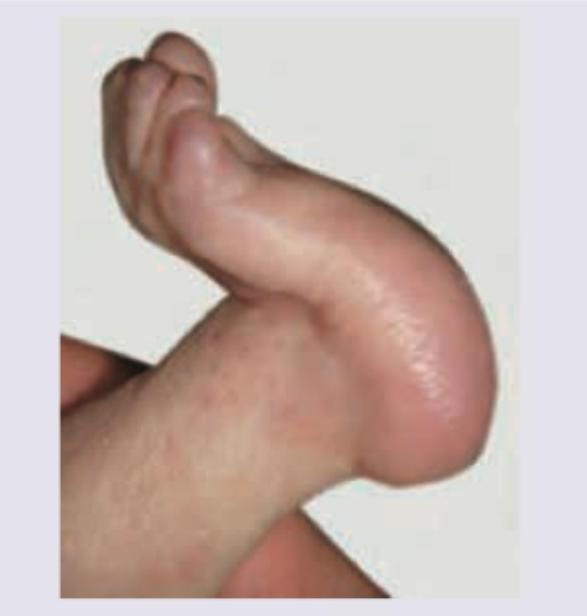
Which of the following syndromes is most classically associated with rocker-bottom feet?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app