
Growth and Development — MCQs

On this page
An infant turns their head toward the sound of a rattle held to the side, outside their initial visual field. By what age can a child perform this activity?

The image shows a child jumping rope. To assess the distinct gross motor milestone of locomotor skipping, the examiner asks the child to move forward using a smooth, alternating step-hop pattern. By what age do most children perform this skill smoothly?
The image shows an infant in the prone position sustaining head control while bearing weight on forearms. This developmental milestone corresponds to which age?

A 5-year-old short stature child is brought for evaluation. Which disease is the most likely diagnosis as depicted by these pictures of the child, foot and retina?

The image shows a child with a positive wrist sign (thumb overlaps the fifth finger when wrapping around the wrist) and the following appearance:
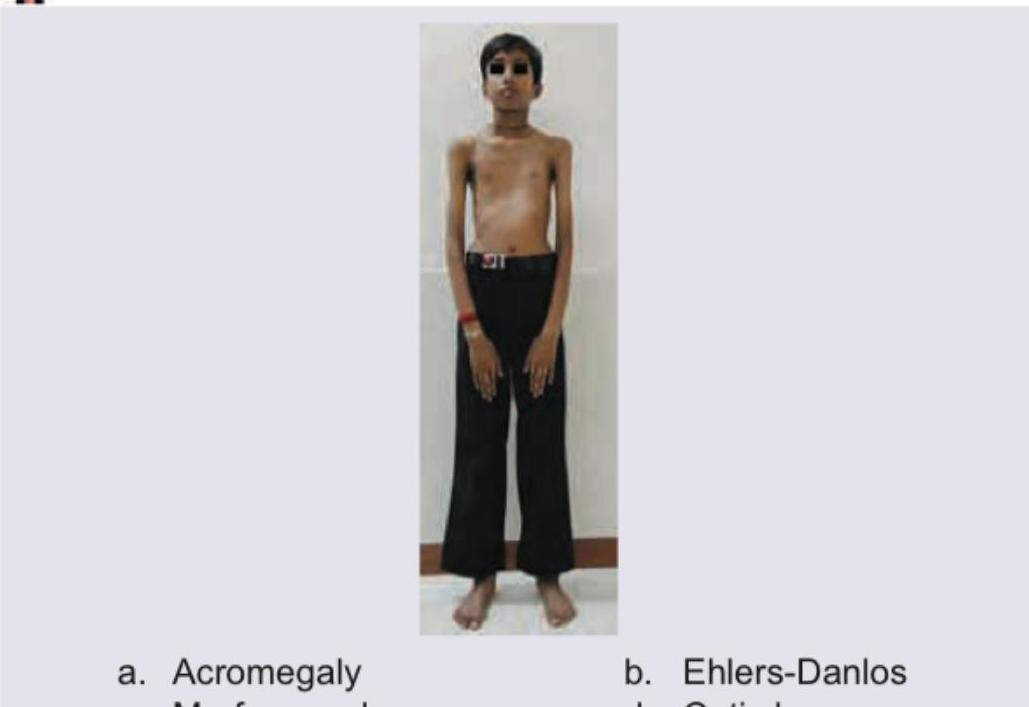
The image shows a child with:

Which of the following is the probable diagnosis in this child with dwarfism, coarse facies. X-ray spine lateral view and X-ray hand is shown?

All of the following can be causes of this enlarged tongue except: (Recent NEET Pattern 2016-17)

The following child has presented with disfigurement and rapidly progressive overgrowth of some body parts. The clinical diagnosis is?

An obese 3-year-old, short stature child with history of hyperphagia, almond eyes and small hands and feet is brought for consultation. On neurological examination hypotonia is noted. IQ is very low. The probable cause is?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app