
Growth and Development — MCQs

On this page
A child makes a tower of 7 cubes at what age?
The following clinical features are seen in which disease?
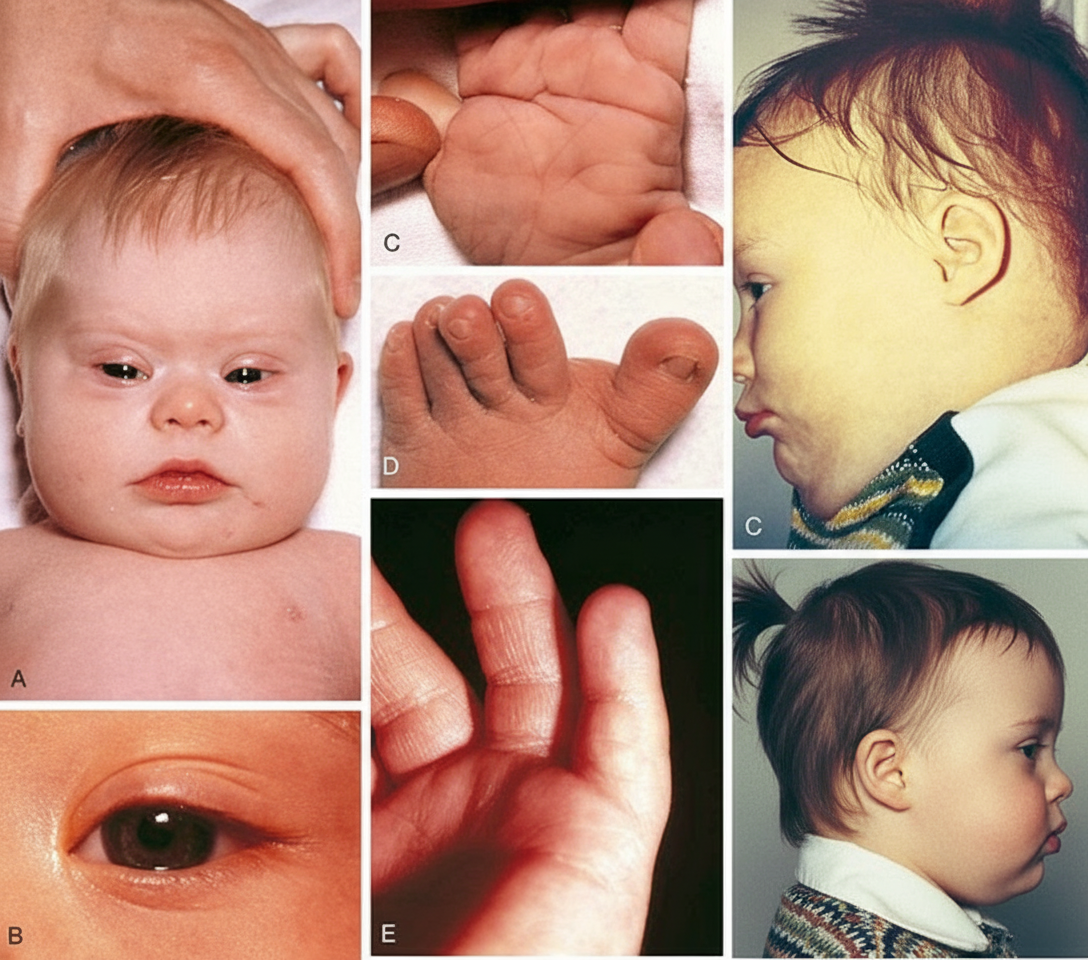
All of the following are true statements about Down syndrome, except:
Delayed dentition is usually considered when there are no teeth by what age?
By what age do teeth typically begin to erupt in primary dentition?
A baby placed in the prone position is able to lift the head and upper chest on extended arms by what age?
What is the normal gain in length for a full-term baby during the first 6 months of life?
Class III malocclusion is seen in all of the following conditions except?
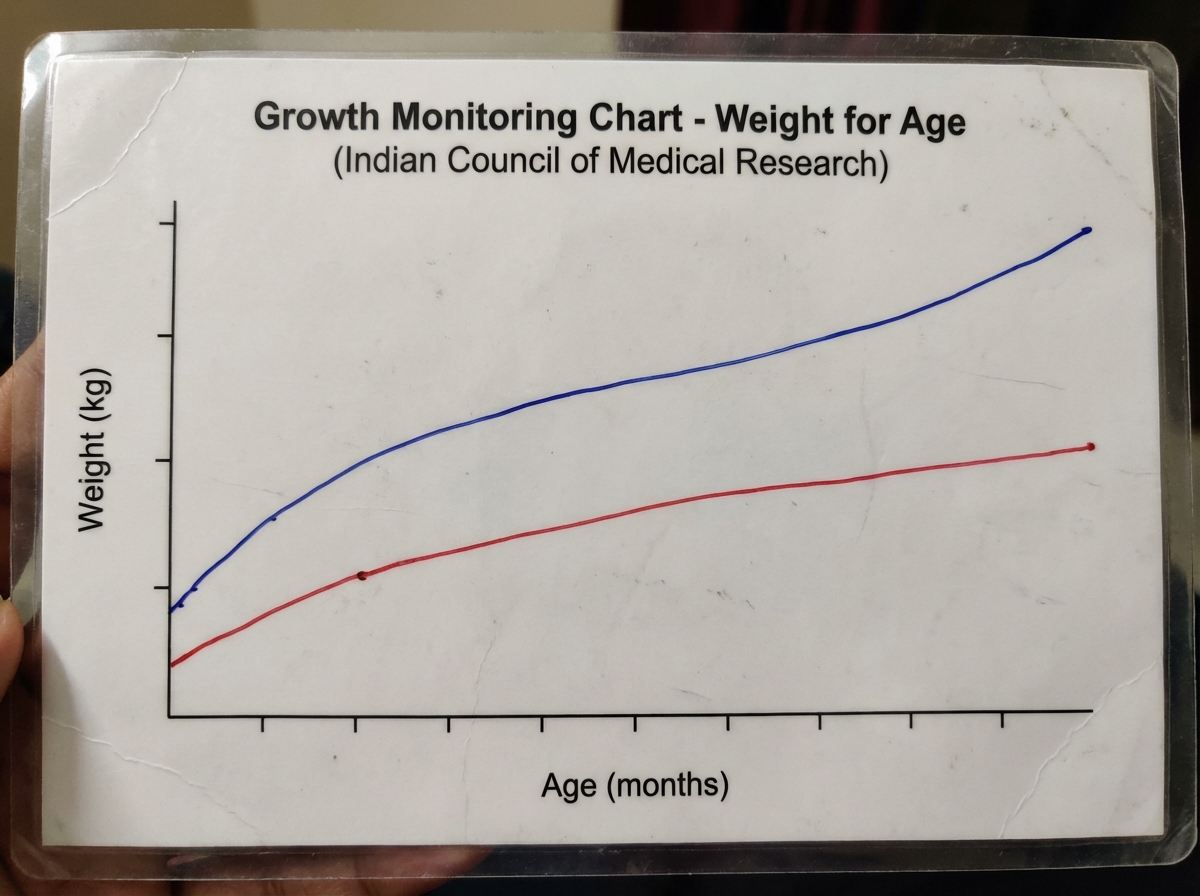
The uppermost line of the card depicted above is equivalent to:
A newborn baby has a head circumference of 35 cm at birth. What will be the optimal head circumference at 6 months of age?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app