
Growth and Development — MCQs

On this page
Social interaction and role-playing typically begin at what age?
How many permanent teeth are typically present in an 8-year-old child?
All of the following social milestones develop at the age of 24 months except:
What is the average gain in length for a child over the first 4 years of life?
A 5-year-old boy told his mother that he had an accident with his bicycle because he was thinking of taking some money from his mother. This type of reasoning is known as?
Which of the following is not a usual feature of Noonan syndrome?
Triangular facies is indicative of which syndrome?
All of the following disorders are associated with a wide anterior fontanelle except?
What is the sequence in which the following developmental milestones are attained?
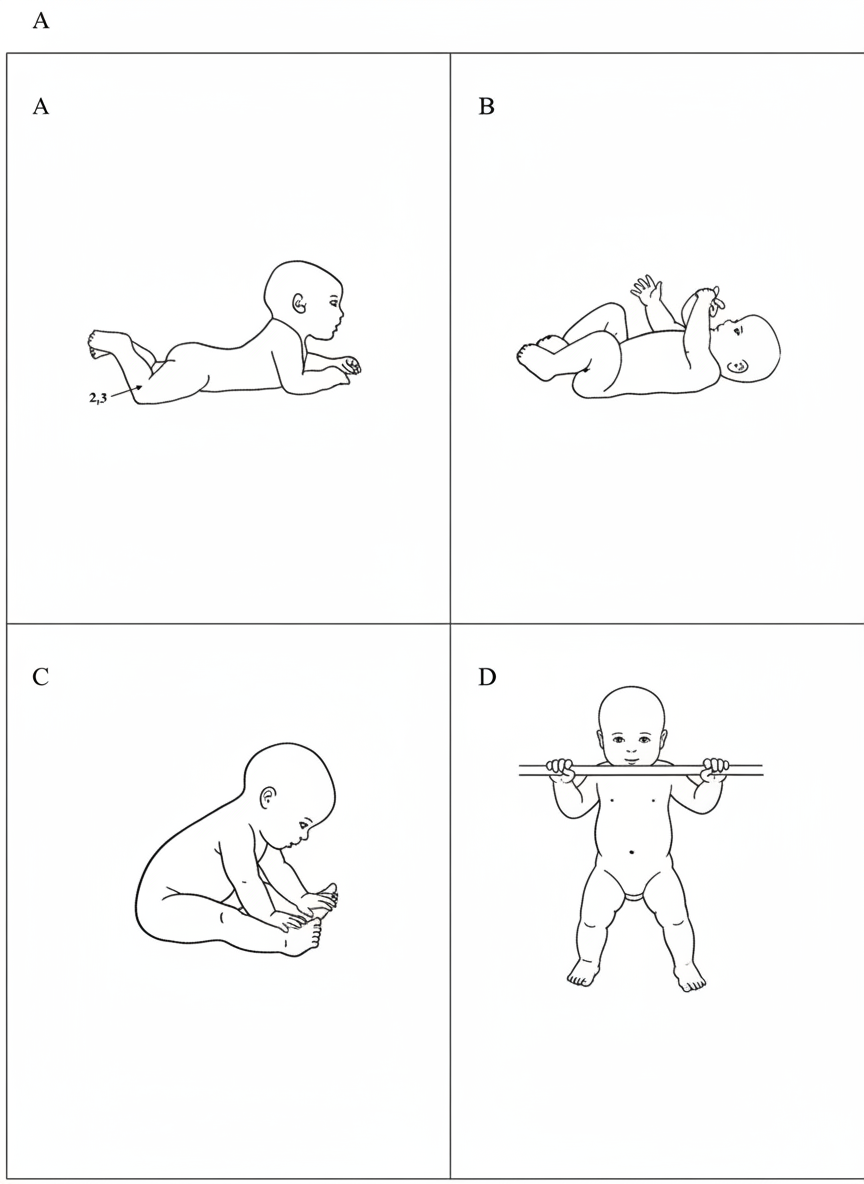
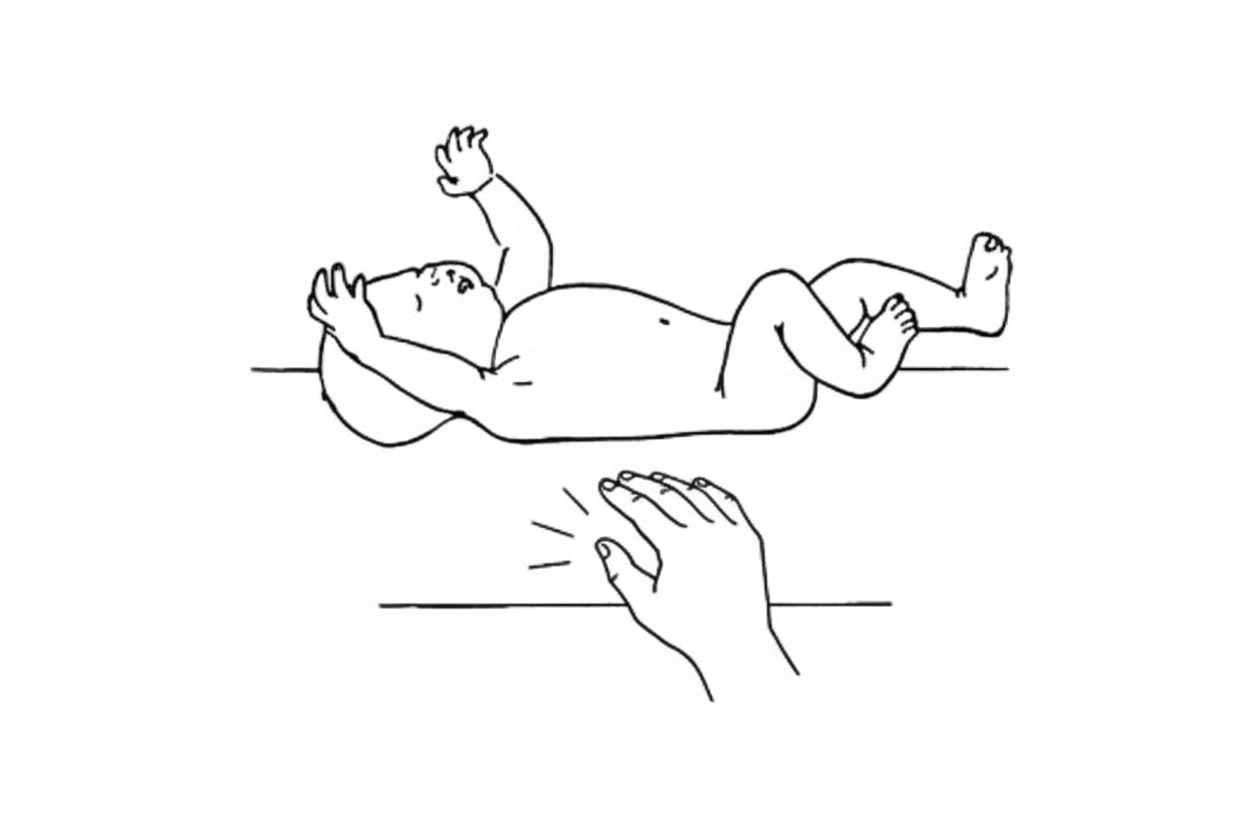
Persistence of the following beyond 6 months of age indicates what?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app