
Growth and Development — MCQs

On this page
Which of the following findings is NOT typically seen in Prader-Willi syndrome?
A bulging anterior fontanelle is seen in which of the following conditions?
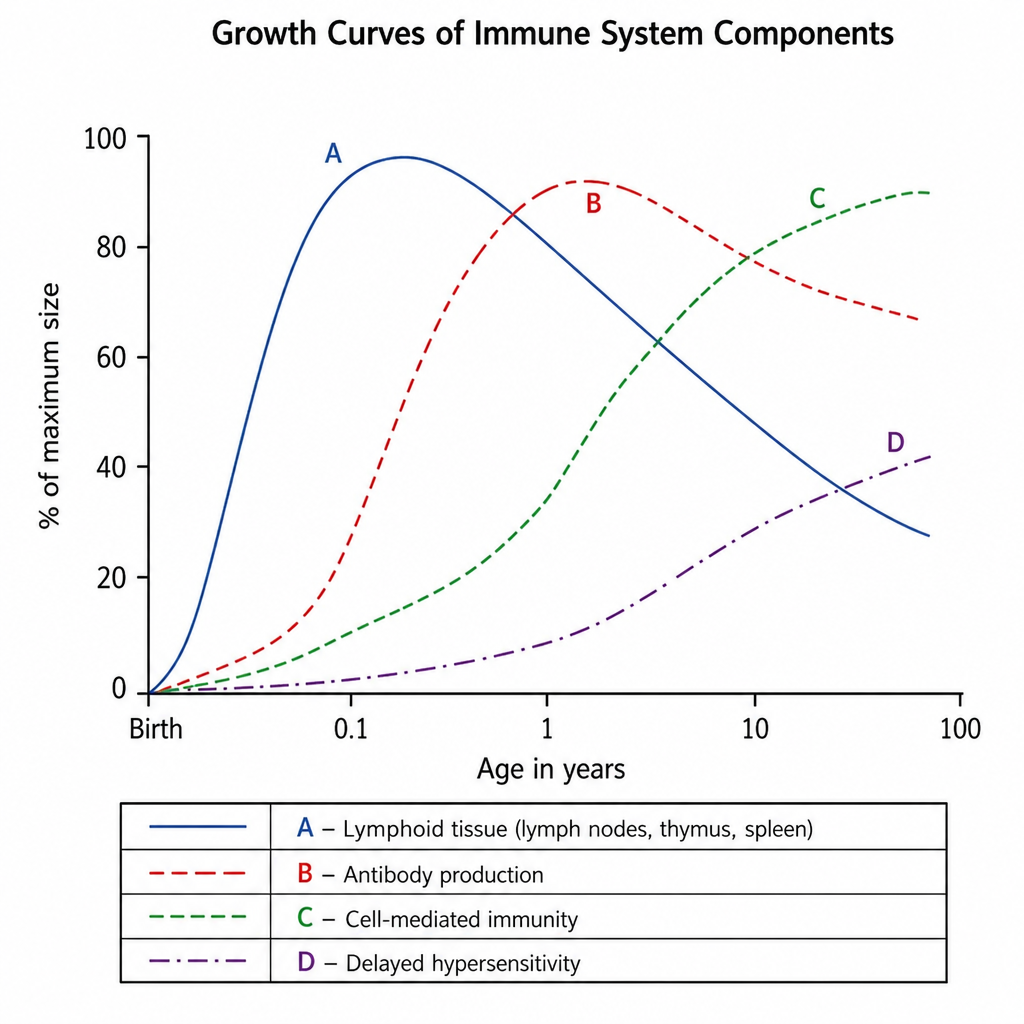
Which of the following curves denotes the lymphoid growth curve?
A child presents with bilateral downslanting palpebral fissures, malar hypoplasia, micrognathia, and external ear anomalies. What is the most likely condition?

At what age does a child typically begin to smile in response to social stimuli?
The anterior fontanelle typically closes by which age?
What is the typical increase in height of a child from 1 to 3 years of age?
An infant can regard his parent's face, follow to midline, lift his head from the examining table, smile spontaneously, and respond to a bell. He does not yet regard his own hand, follow past midline, nor lift his head to a 45-degree angle off the examining table. Which of the following is the most likely age of the infant?
What is the ponderal index of a child with weight 2000 g and height 50 cm?
Which of the following is a characteristic of Tanner Stage 2 (SMR-2) in boys?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app