
Growth and Development — MCQs

On this page
At what age does the intracellular fluid (ICF) and extracellular fluid (ECF) ratio in a child become equal to that of an adult?
Non-appearance of social smile by how many weeks is considered abnormal?
All of the following may occur in Down's syndrome, except:
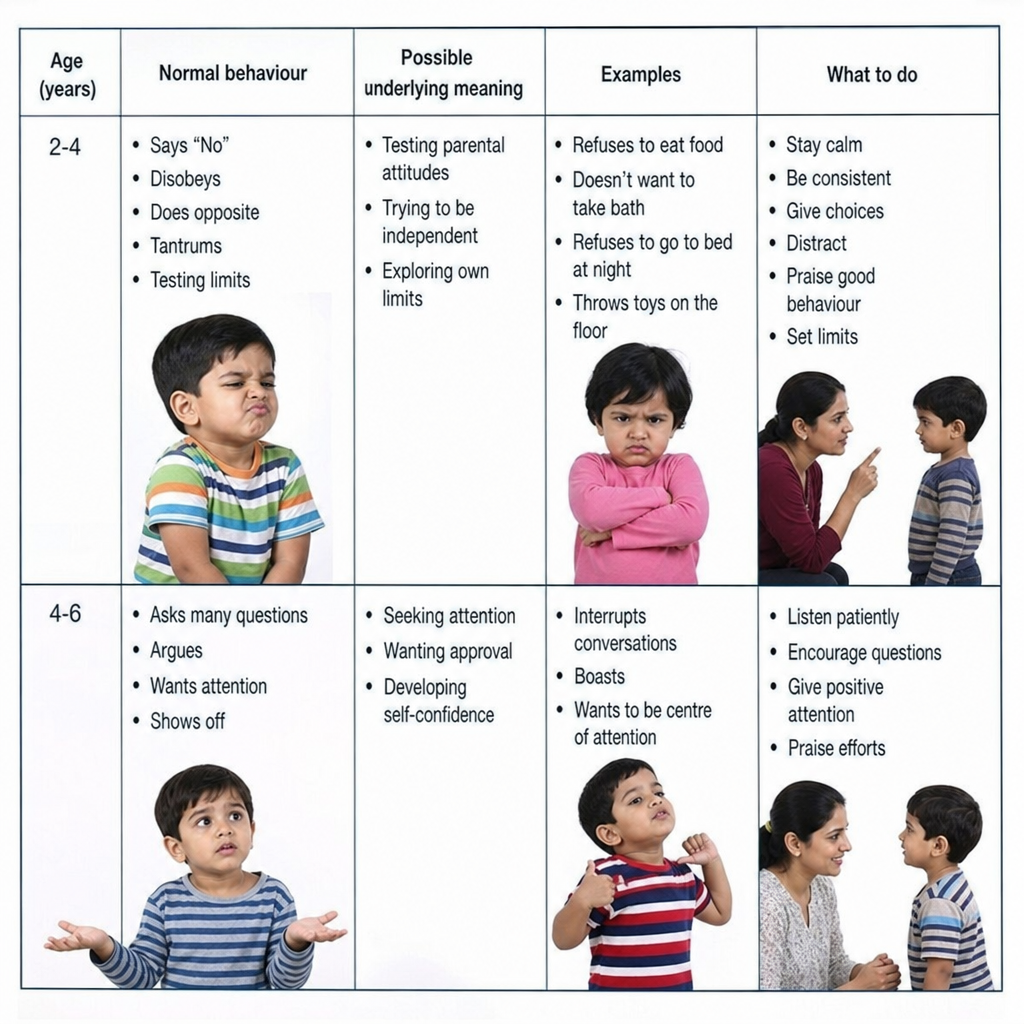
A child between 2-4 years of age exhibiting behaviours such as saying no, tantrums, disobedience, and limit testing indicates:
A child can typically draw a horizontal line by what earliest age?
Which milestone is typically achieved by the age of 4 months?
A 2-year-old child can typically perform which of the following actions?
All are true regarding WHO growth charts, EXCEPT:
What percentage of birth weight does a newborn typically lose in the first week of life?
At what age does a child typically begin to transfer a rattle from one hand to another?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app