
Growth and Development — MCQs

On this page
A 4-year-old baby is having a large face, large jaw, large ears, and macroorchidism. What is the diagnosis?
At what age is a child typically able to tell stories?
Closure of the anterior fontanelle is delayed in all of the following conditions except?
Which of the following is true about Tanner stage 3?
Which of the following signs would warrant further evaluation of developmental status in a healthy 12-week-old infant?
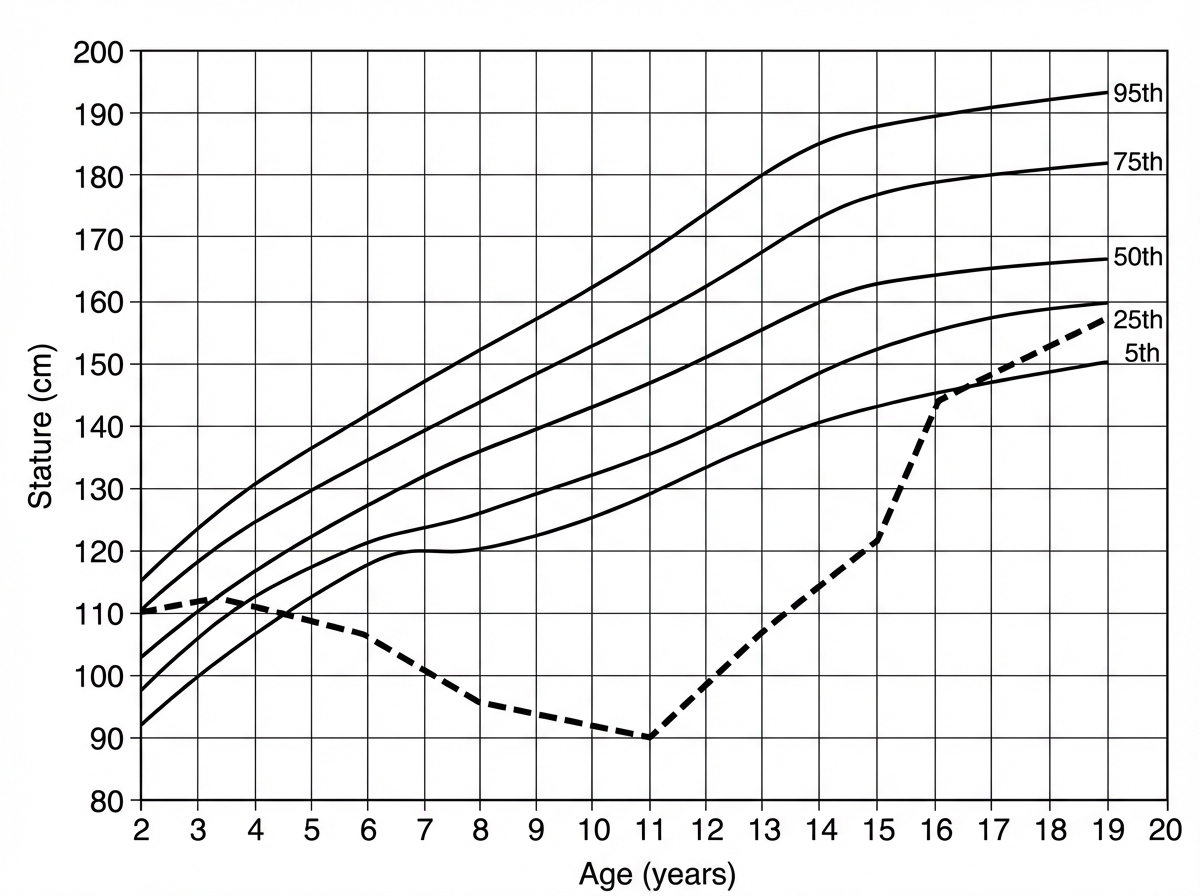
What condition does the dotted line in the following growth chart represent?
A baby can follow an object till 180 degrees and can hold their neck, and can sit without support. What is the approximate age of the baby?
A 10-year-old male, who is mentally retarded, is able to carry out activities of daily living, including feeding and dressing himself. On physical examination, he has brachycephaly and oblique palpebral fissures with prominent epicanthal folds. The palm of each hand shows a transverse crease. On auscultation of the chest, there is a grade III/IV systolic murmur. Which of the following diseases is he most likely to develop by the age of 20?
All of the following may occur in Noonan's syndrome, EXCEPT:
What is the percentile BMI used to define underweight?
Practice by Chapter
Normal Growth Parameters
Practice Questions
Developmental Milestones
Practice Questions
Puberty and Adolescent Development
Practice Questions
Growth Disorders
Practice Questions
Failure to Thrive
Practice Questions
Developmental Screening and Assessment
Practice Questions
Developmental Delays
Practice Questions
Growth Charts and Monitoring
Practice Questions
Short Stature
Practice Questions
Tall Stature
Practice Questions
Precocious and Delayed Puberty
Practice Questions
Psychosocial Development
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app