
Normal Growth Parameters — MCQs

A 5-year-old has the following anthropometry findings: Weight/age < -3.2 SD, Height/age < -2.5 SD, Weight/height < -1.7 SD. What is the most likely diagnosis?
Anthropometric assessment, which does not show much change over a period of 1-4 years, is characteristic of:
Type of growth chart used by anganwadi workers (ICDS) for growth monitoring is:
In anthropometric assessment, which of the following does not show much change in 1-4 years ?
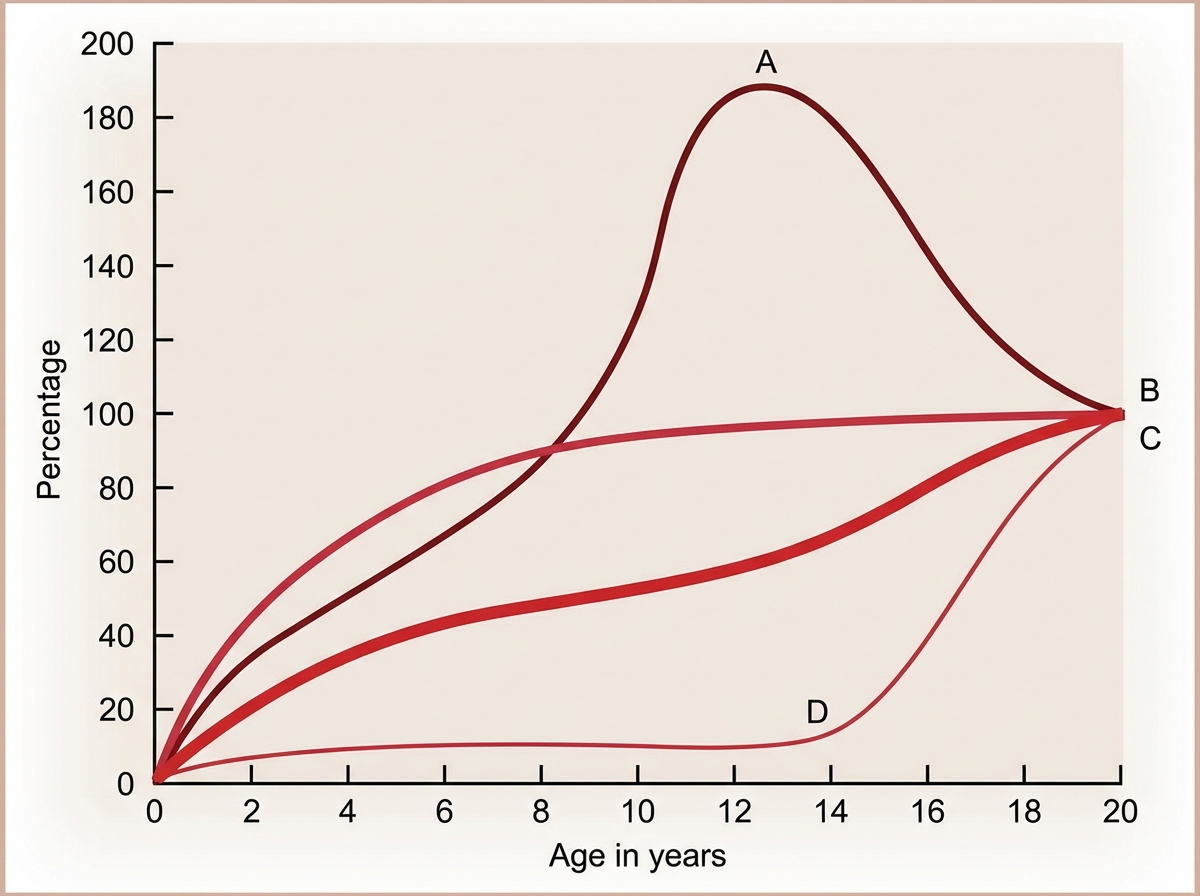
The Image shows the growth curve of different organs with age. Identify A in the graph.
What is the true statement regarding an 'at-risk baby'?
Which of the following is not a feature of hypothyroidism in infancy?
Deficit in weight for height in a 3-year-old child indicates a type of malnutrition:
The following are recognized signs and symptoms of raised intracranial tension in a 9-month-old infant, except which of the following?
A child presents with short stature. His bone age is less than chronological age. The height of his parents is normal. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app