
Gastroenterology — MCQs

On this page
6 year old drowsy child came in emergency with history of vomiting, loose motion for 3 days. On examination he had sunken eye, hypothermia, skin on pinching takes time to revert. Diagnosis
The most common congenital esophageal anomaly is which of the following?
A 4-week-old boy is brought to your OPD by his mother because he has had increasing amounts of vomiting over the past week. Initially it started as "spitting up" after a few meals a day, but now the baby is having projectile vomiting after every meal. She says the vomitus is non-bloody and non-bilious and the baby appears hungry after he vomits. This is her first child and she is not sure if this is normal. Physical examination is unremarkable. Laboratory studies show: Sodium: 140 mEq/L Potassium: 3.0 mEq/L Chloride: 87 mEq/L Bicarbonate: 30 mEq/L At this time the most appropriate next step is to
Amount of ORS to be given in the first 4 hours to a child with some dehydration is
Persistent diarrhoea is defined as diarrhoea lasting more than?
A 10-year-old child presents with recurrent episodes of blood in stool. On examination, his lips show pigmented macules. He may be suffering from?
A 3-year-old child is evaluated by a pediatrician for poor growth despite excessive food intake. The mother reports that the child's stools are bulky, foul-smelling, and difficult to flush because they float. Determination of which of the following would most likely be diagnostic in this case?
Which of the following metabolic derangements is associated with congenital pyloric stenosis?
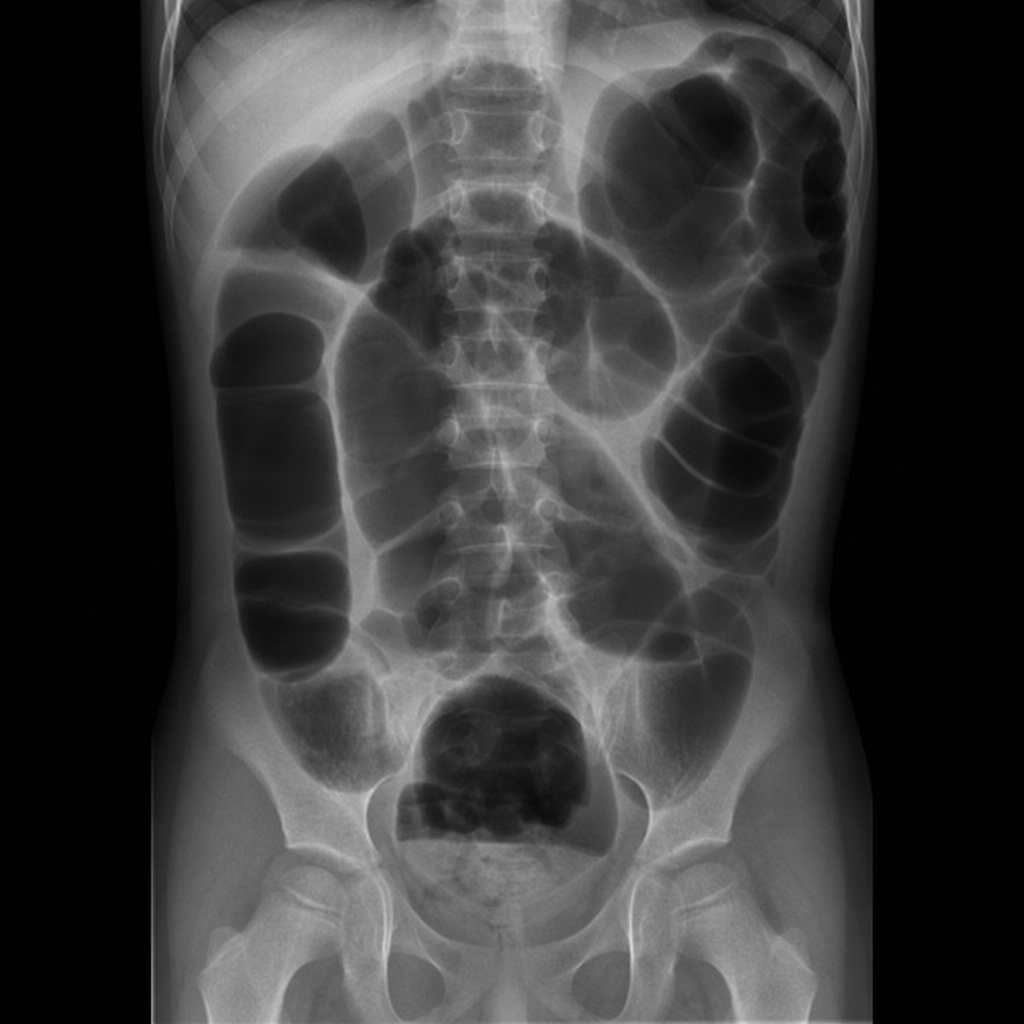
A 4-year-old boy presents with a history of constipation since the age of 6 months. His stools, produced every 3 to 4 days, are described as large and hard. His growth velocity is normal. Physical examination is normal; rectal examination reveals a large ampulla, poor sphincter tone but present anal wink, and stool in the rectal vault. The plain film of his abdomen is shown. Which of the following is the most appropriate next step in the management of this child?
The most common cause of fresh bleeding per rectum in a 5-year-old child is:
Practice by Chapter
Gastroesophageal Reflux
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Celiac Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Acute and Chronic Diarrhea
Practice Questions
Constipation and Encopresis
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Intestinal Obstruction
Practice Questions
Liver Diseases in Children
Practice Questions
Pancreatic Disorders
Practice Questions
Pediatric Nutritional Support
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app