
Gastroenterology — MCQs

On this page
Most common cause of intestinal obstruction in childhood is:
Consider the following features: 1. Visible gastric peristalsis 2. Bilious vomiting 3. Palpable tumour 4. Melena Which of these is/are feature/features of infantile hypertrophic pyloric stenosis?
An eight month old male child is brought to the emergency with recurrent episodes of screaming and drawing up of legs. The child appears to be listless in between the attacks. Local examination of abdomen reveals feeling of emptiness in the right iliac fossa and blood stained mucus is found on the finger on rectal examination. The most probable clinical diagnosis in this child is
A child presents with itchy lesions and diarrhea and has been advised to follow a gluten-free diet. What is the most likely etiology of this condition?
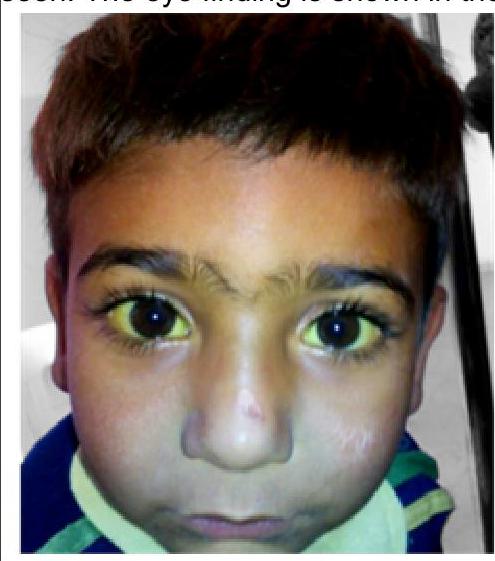
An 11-year-old boy was brought to the outpatient clinic with intention tremor and poor scholastic performance. His sister has similar complaints. On examination, hepatomegaly is seen. The eye finding is shown in the image. What is the probable diagnosis?
A 6-year-old child is brought with high fever with rigors for 5 days with pain in right hypochondrium. On examination, the patient is anicteric and tenderness is noted in right upper quadrant. What is the best investigation for this case?
Most common cause of cholestatic jaundice in newborn is
Acquired megacolon in children is most commonly due to-
In a child, which of the following diseases is commonly misdiagnosed as appendicitis?
A baby with diarrhea presented with restlessness but is able to drink water. Skin turgor goes back in 2 seconds. The baby is communicating properly. What is the best management?
Practice by Chapter
Gastroesophageal Reflux
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Celiac Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Acute and Chronic Diarrhea
Practice Questions
Constipation and Encopresis
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Intestinal Obstruction
Practice Questions
Liver Diseases in Children
Practice Questions
Pancreatic Disorders
Practice Questions
Pediatric Nutritional Support
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app