
Gastroenterology — MCQs

On this page
A 6-week-old infant presents with a history of non-bilious, non-projectile vomiting starting at 3 weeks of age. The infant's abdominal examination is normal. Which of the following is the most likely diagnosis?
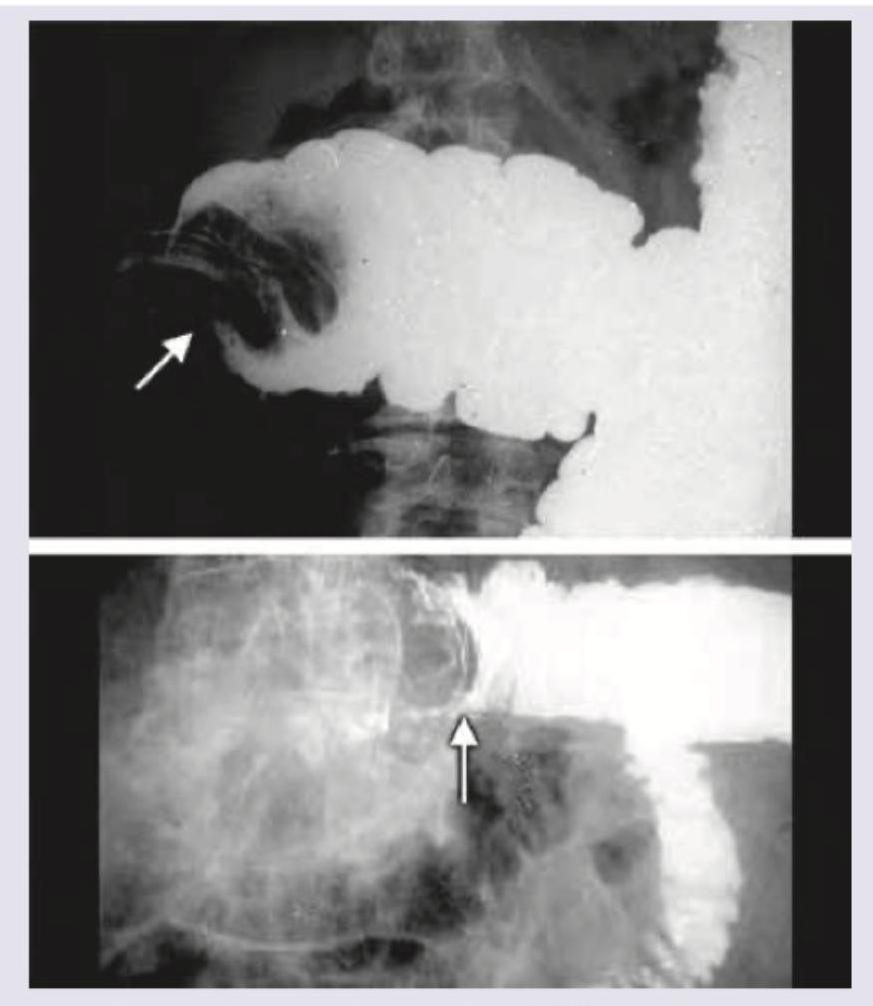
A 4-week-old baby presents with non-bilious vomiting and abdominal distension. The radiological image is shown. Among the clinical features, which is the most specific physical examination finding in reaching the diagnosis of this condition?
All of the following statements regarding this image are true except:
A baby presents with colicky abdominal pain. Mother gives a history of bloody stools. All the statements regarding this condition are true except:
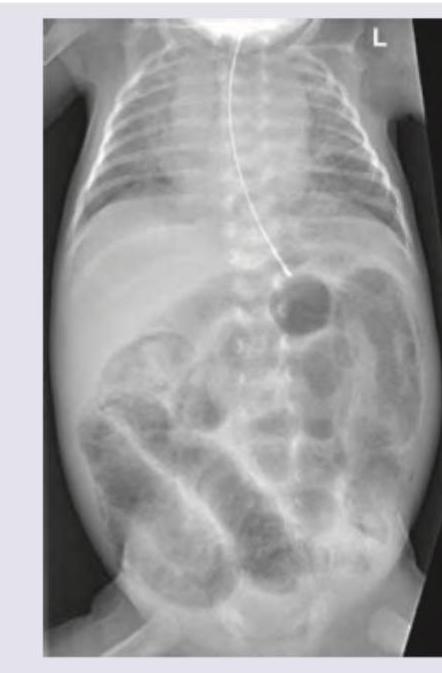
A baby on day 4 of its birth presents with repeated vomiting. The vomiting is bilious in nature. What is the most possible diagnosis as per the infantogram?

A 6-year-old child is brought with the following lesion. In which gastrointestinal organ do hamartomatous polyps most commonly develop in this condition?

A 2-day-old neonate with persistent jaundice, elevated direct bilirubin, dark urine, hepatomegaly, and persistently acholic stools has passed stool of the color shown in the image. Which of the following best describes the clinical possibility?

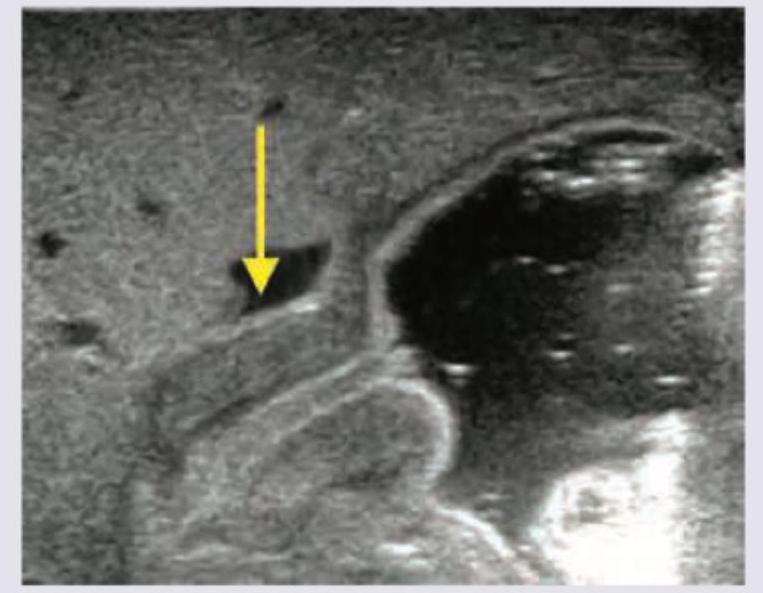
A newborn presents with bilious vomiting on the first day of life. X-ray abdomen shows:
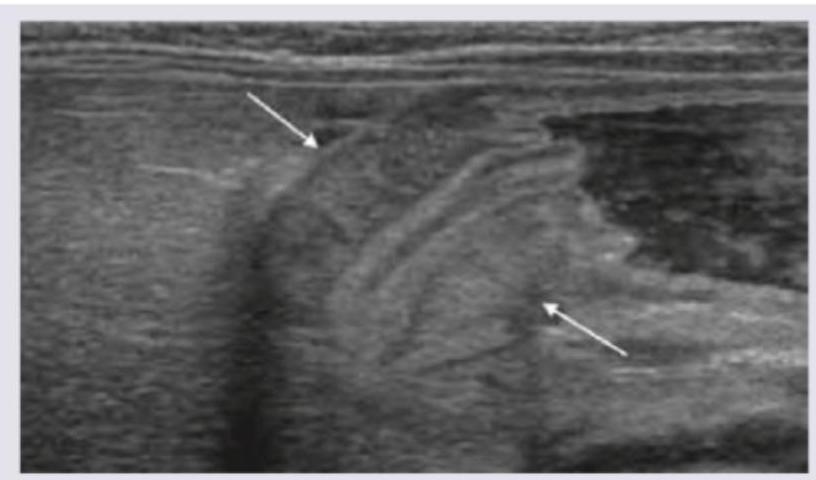
Neonate is brought at 3 weeks of age, with projectile vomiting. USG was performed and is shown below. When can the abdominal mass in this condition be best palpated?
Which of the following statements are correct regarding the management of gastrointestinal bleeding in children? I. Somatostatin or octreotide infusion should be given for at least 7 days after stoppage of initial bleeding to prevent rebleeding II. Endoscopic Sclerotherapy (EST) involves endoscopic injection of N -butyl-2-cyanoacrylate or iso-butyl-2-cyanoacrylate III. EST has upto 90 % efficacy in controlling acute bleeding IV. Following an episode of acute variceal bleeding, all patients should receive secondary prophylaxis to prevent rebleeding Select the answer using the code given below :
Practice by Chapter
Gastroesophageal Reflux
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Celiac Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Acute and Chronic Diarrhea
Practice Questions
Constipation and Encopresis
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Intestinal Obstruction
Practice Questions
Liver Diseases in Children
Practice Questions
Pancreatic Disorders
Practice Questions
Pediatric Nutritional Support
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app