
Gastroenterology — MCQs

On this page
A 10-year-old male child presents with a 2-day history of pain in the left hypochondrium. His Hb is 9.69%. His mother reports episodes of passing black-colored stools occurring 7 days prior and on 2-3 occasions over the past 2 years. During these episodes, he experienced fatigability while playing and was unable to keep up with his peers. Which of the following findings will be most helpful in arriving at a clinical diagnosis?
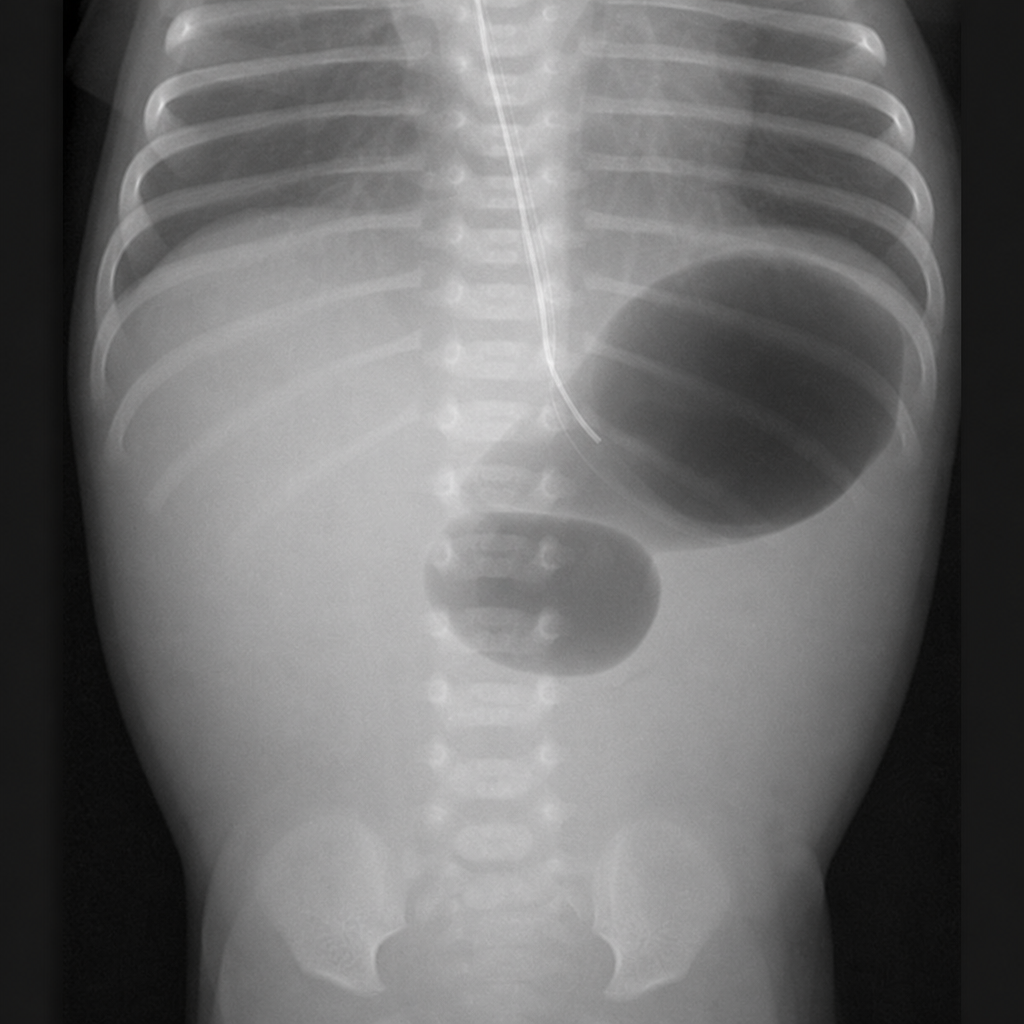
At the time of delivery, a woman is noted to have a large volume of amniotic fluid. At 6 hours of age, her baby begins regurgitating small amounts of mucus and bile-stained fluid. Physical examination of the infant is normal, and an abdominal x-ray is obtained. Which of the following is the most likely diagnosis of this infant's disorder?
A 2-year-old child presented with hepatomegaly. Which of the following is NOT a potential cause?
What is the recommended amount of Oral Rehydration Solution (ORS) to be given to a child weighing 4 kg who has diarrhea?
Celiac disease in children is most commonly associated with which of the following?
Childhood cholelithiasis is seen in which of the following conditions?
Which of the following individuals shows susceptibility to dental caries?
What is the most common cause of diarrhea in children?
All of the following are acceptable home-available fluids for acute diarrhea except:
An infant presents with 15-20 watery stools for 9 days. Along with Zinc supplementation, what additional management should be provided?
Practice by Chapter
Gastroesophageal Reflux
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Celiac Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Acute and Chronic Diarrhea
Practice Questions
Constipation and Encopresis
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Intestinal Obstruction
Practice Questions
Liver Diseases in Children
Practice Questions
Pancreatic Disorders
Practice Questions
Pediatric Nutritional Support
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app