
Gastroenterology — MCQs

On this page
All of the following are true about Reye's syndrome, EXCEPT?
The following sign is seen in which of the following anomaly?
Which of the following is NOT a gastrointestinal disturbance seen in cystic fibrosis?
In cystic fibrosis of the pancreas, which part of the small intestine is most commonly affected?
What is the minimum duration of stool frequency and/or fluidity to define persistent diarrhea in infants?
Dehydration in a child with diarrhea, thirst present, and absent tears is classified as which of the following?
A baby born at term develops abdominal distention in the first week of life. Meconium ileus is diagnosed. Subsequently, the infant has persistent steatorrhea and fails to develop normally. Which of the following laboratory test findings is most likely related to the infant's underlying disease?
An 8-year-old boy presents with a history of abdominal pain that is exacerbated during the week and lessens on weekends. His growth and development are normal. He has one soft stool daily without painful defecation. Physical examination is unremarkable, and laboratory investigations including stool for occult blood, CBC, urinalysis, and chemistry panel are within normal limits. What is the most appropriate next step in managing this patient?
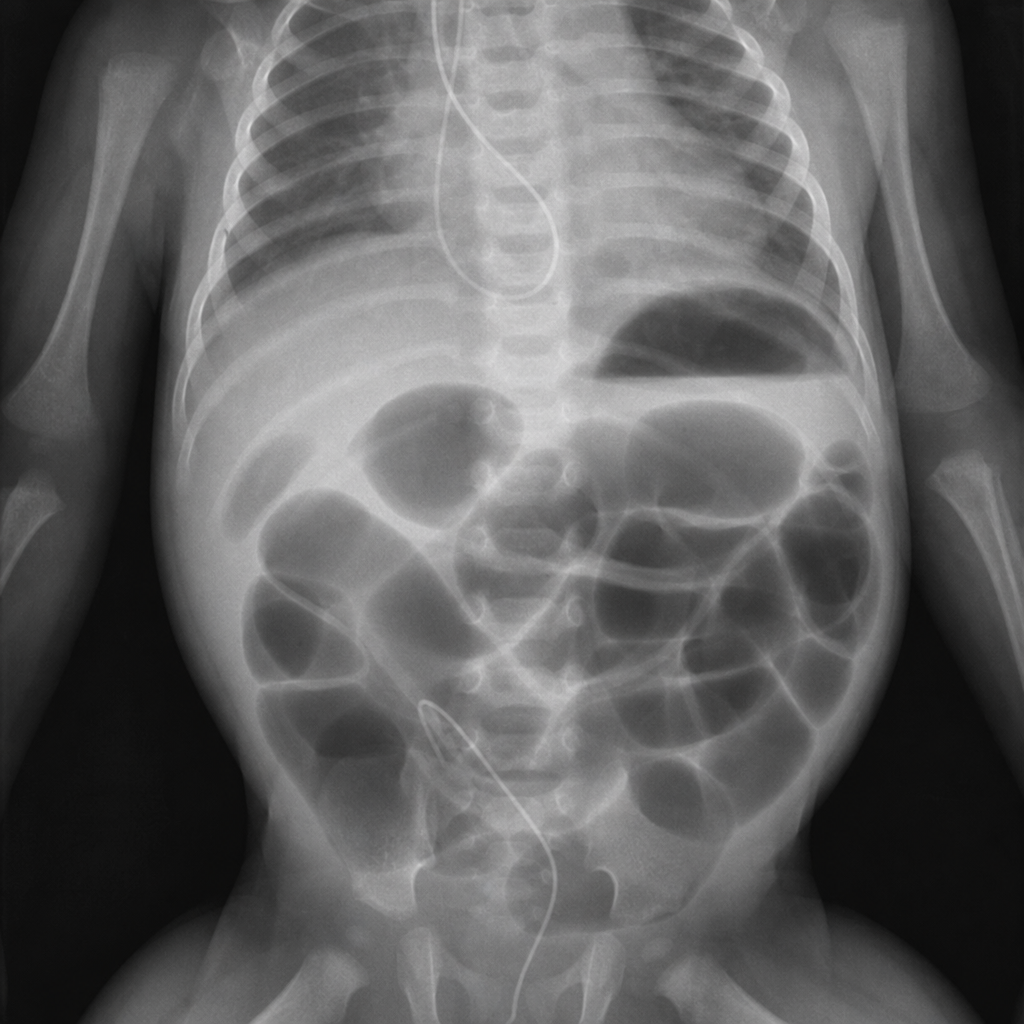
A 6-year-old boy presents with a 3-month history of soiling his underwear almost daily, despite being toilet trained at 2 years of age without difficulty. He has also experienced ongoing constipation for the last 2 years and frequently states, "I didn't know I had to go." He is otherwise healthy, performing well in school, and has a stable home environment. Examination reveals stool in the rectal vault. A plain radiograph of his abdomen is provided. What is the most appropriate initial management for this condition?

A 2-year-old boy presented with abdominal distension, chronic diarrhoea, severe anaemia, and failure to thrive. Which of the following is the investigation of choice?
Practice by Chapter
Gastroesophageal Reflux
Practice Questions
Peptic Ulcer Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Celiac Disease
Practice Questions
Malabsorption Syndromes
Practice Questions
Acute and Chronic Diarrhea
Practice Questions
Constipation and Encopresis
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Intestinal Obstruction
Practice Questions
Liver Diseases in Children
Practice Questions
Pancreatic Disorders
Practice Questions
Pediatric Nutritional Support
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app