
Gastroesophageal Reflux — MCQs

A 3-month-old with projectile vomiting and olive-shaped mass in abdomen is diagnosed with?
A 24-day-old neonate presents with projectile vomiting and failure to gain weight. What is the most likely diagnosis?
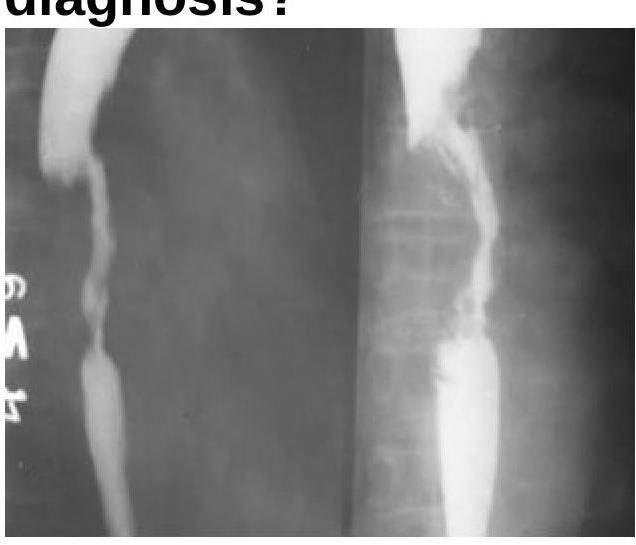
A 55-year-old male presents with a history of dysphagia with vomiting of undigested food throughout the day, weight loss, and appears emaciated and dehydrated. No mass is palpable per abdomen. After appropriate diagnostic workup reveals a benign esophageal stricture, the most appropriate definitive management is:
The Barium Swallow examination shows a filling defect in the esophagus. What is the most probable diagnosis?
A 40-year-old male with gastroesophageal reflux disease (GERD) is found to have Barrett's esophagus with low-grade dysplasia on endoscopy. What is the most appropriate initial pharmacological treatment for this condition?
A 60-year-old man presents with foul breath and regurgitates food eaten 3 days ago. What is the most likely diagnosis?
The most common complication of Zenker's diverticulum is:
False statement about Barrett esophagus is:
Adenocarcinoma of the esophagus is commonly found in patients with which of the following conditions?
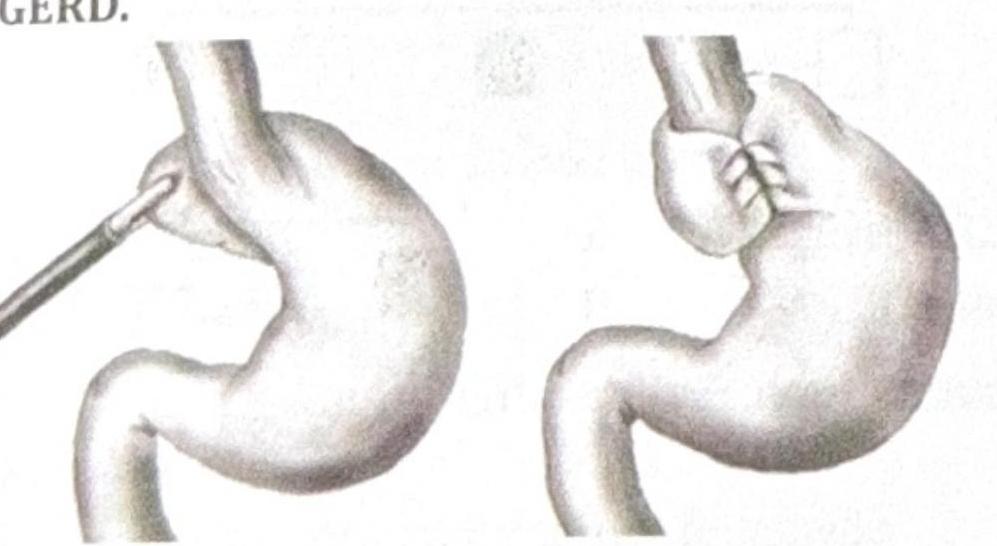
Identify the procedure shown in the image, which is performed in a patient with recurrent GERD.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app