
Endocrinology — MCQs

On this page
Which statin is indicated for an 8-year-old child diagnosed with heterozygous familial hypercholesterolemia?
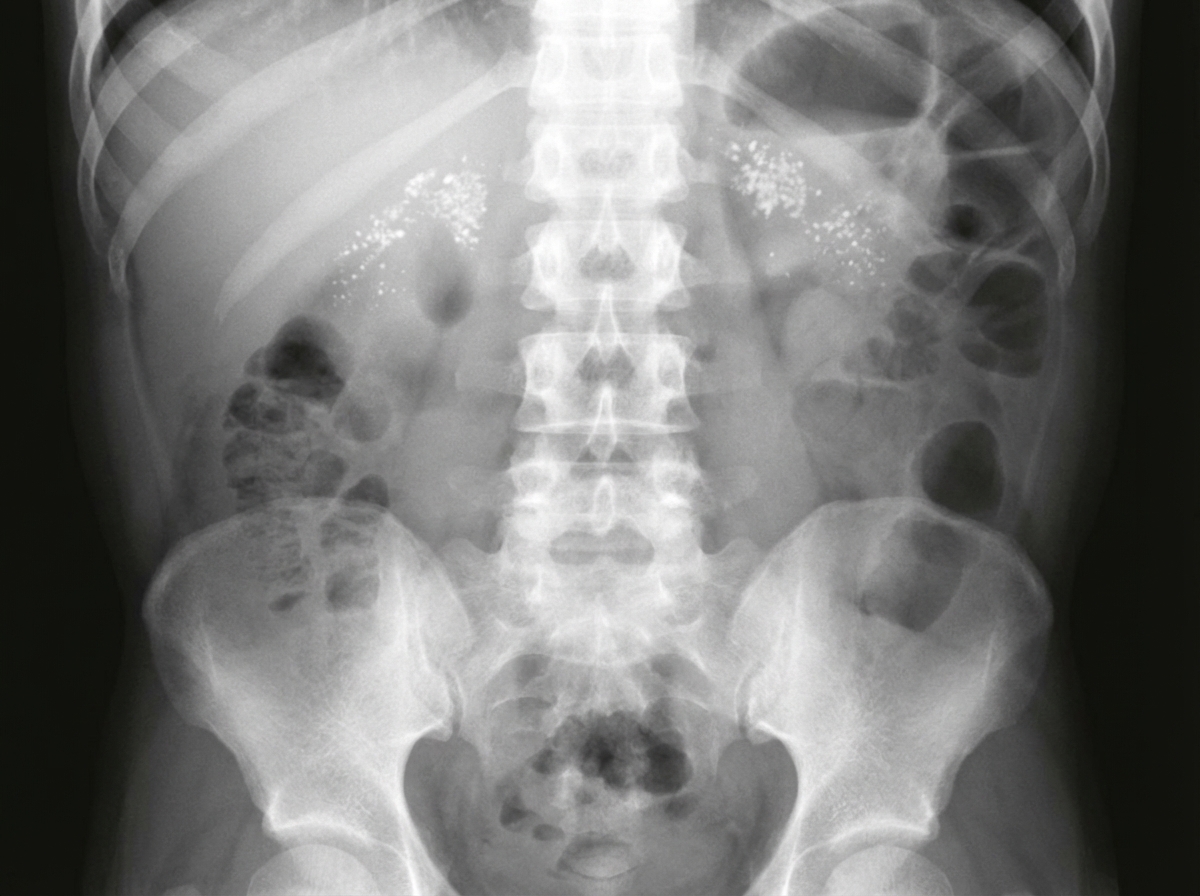
A 2-month-old infant presents with failure to thrive, recurrent emesis, hepatosplenomegaly, and adrenal insufficiency. Adrenal calcification is noted radiologically. What is the most probable diagnosis?
Which of the following is NOT a known cause of precocious puberty?
Precocious puberty is seen in which of the following conditions?
An infant presents with failure to thrive and abdominal distension. His X-ray chest and abdomen showed findings suggestive of a diagnosis. What is the diagnosis?
Which of the following is NOT true about congenital hypothyroidism?
A 2-week-old infant presents with feeding difficulties, somnolence, failure to thrive, and constipation. Blood studies reveal low T4 and high TSH. If appropriate therapy is not promptly instituted, which of the following complications would most likely occur?
A cherry red spot is seen in which of the following conditions?
Late onset of puberty in the male is defined as:
Which of the following statements is not true about Turner's syndrome?
Practice by Chapter
Disorders of Growth
Practice Questions
Thyroid Disorders
Practice Questions
Disorders of Puberty
Practice Questions
Adrenal Disorders
Practice Questions
Diabetes Mellitus in Children
Practice Questions
Disorders of Calcium and Phosphate Metabolism
Practice Questions
Disorders of Sexual Development
Practice Questions
Hypoglycemia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Pituitary Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app