
Endocrinology — MCQs

On this page
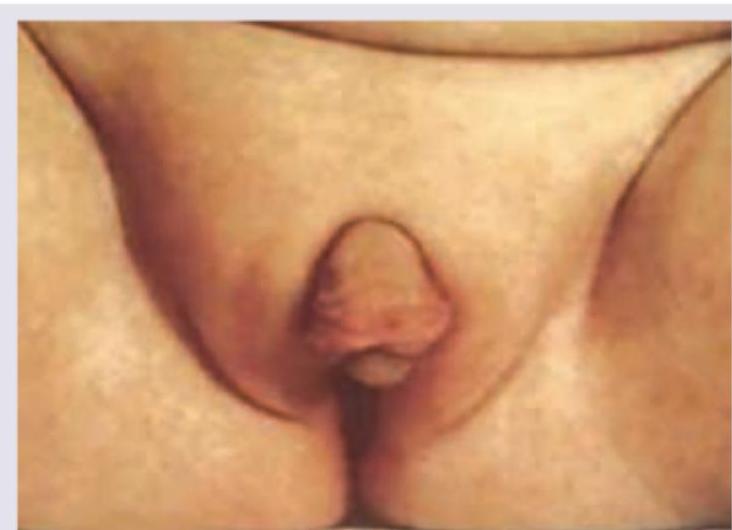
Which is true about an infant with failure to thrive, ambiguous genitalia, dehydration, hypotension, hyponatremia, and hyperkalemia consistent with a salt-wasting crisis due to 21-hydroxylase deficiency?
Which of the following are causes of hypocalcemia in a child? I. Hypomagnesemia II. Hypophosphatemia III. Metabolic acidosis IV. Pseudohypoparathyroidism Select the correct answer using the code given below :
The clinical features of Turner Syndrome in girls include the following except:
Which of the following are causes of GnRH dependent precocious puberty? 1. Constitutional 2. Tubercular Encephalitis 3. McCune-Albright syndrome 4. Primary hypothyroidism
Which test is not required for Turner mosaic syndrome?
In a newly diagnosed case of a sick child with type 1 diabetes mellitus (DM), insulin was given. Which of the following will increase:
Cretinism is -
Hyperthyroidism in children is not associated with:
Screening for nephropathy in prepubertal children with type 1 DM should be initiated after how many years of disease onset?
An eight-year-old girl presented by her mother with sexual precocity. She may have the following disorder:
Practice by Chapter
Disorders of Growth
Practice Questions
Thyroid Disorders
Practice Questions
Disorders of Puberty
Practice Questions
Adrenal Disorders
Practice Questions
Diabetes Mellitus in Children
Practice Questions
Disorders of Calcium and Phosphate Metabolism
Practice Questions
Disorders of Sexual Development
Practice Questions
Hypoglycemia
Practice Questions
Obesity and Metabolic Syndrome
Practice Questions
Pituitary Disorders
Practice Questions
Multiple Endocrine Neoplasia Syndromes
Practice Questions
Endocrine Emergencies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app