
Endocrine Emergencies — MCQs

Fluid of choice for shock in a child with severe acute malnutrition + hypoglycemia
A patient with DKA has a pH of 7.1, Na 130, and K 5.5. What is the best initial treatment?
Which of the following is a common finding in patients with Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)?
Which of the following is not true about syndrome of inappropriate antidiuretic hormone secretion (SIADH)?
A 37-week small-for-date neonate is most likely to develop
A child presented to the casualty department with fever, unconsciousness, and papilledema. What is the next step?
A 4-year-old admitted in ward with pneumonia. He develops sudden onset of breathlessness. What is the next step in management?

The image shows a child with virilisation and clitoromegaly. What laboratory finding is typical for this condition, assuming the most common enzyme defect?
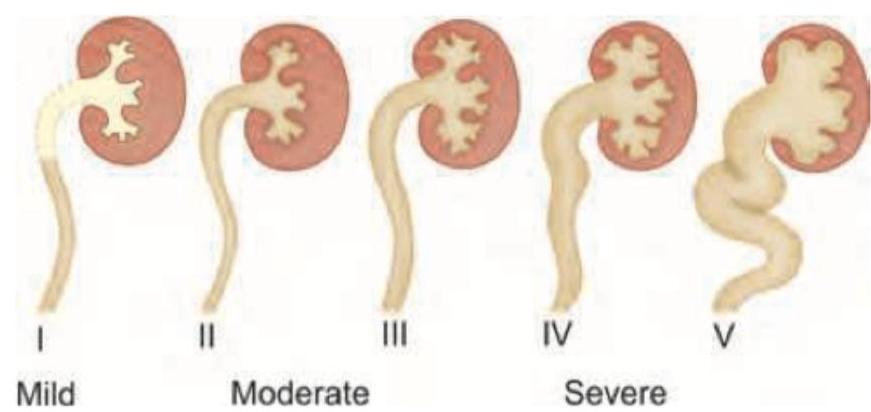
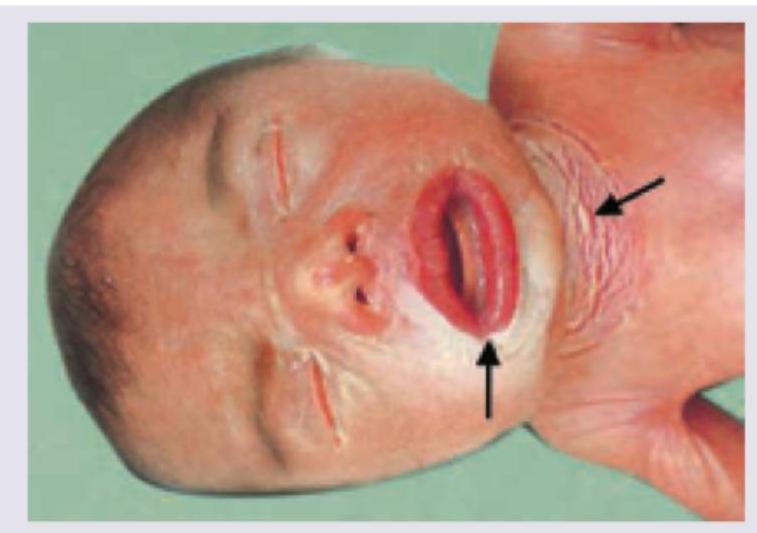
A neonate presents with the condition shown in the image below. This condition has all of the following features EXCEPT:
A 3-week-old female infant presents with ambiguous genitalia and hyperpigmentation of the skin. Laboratory findings include hyponatremia and hyperkalemia. What is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app