
Sleep Disorders — MCQs

Modafinil is approved by FDA for treatment of all except:
Narcolepsy is associated with?
A 7-year-old girl is reported by the parents as waking up in the night screaming, and she sits up in bed frightened. She does not respond to questions and after 2 or 3 minutes she goes back to sleep. She has no memory of these events the following morning. Which of the following is the most likely diagnosis?
A child presents with complaints of bed wetting. What is the first line of treatment?
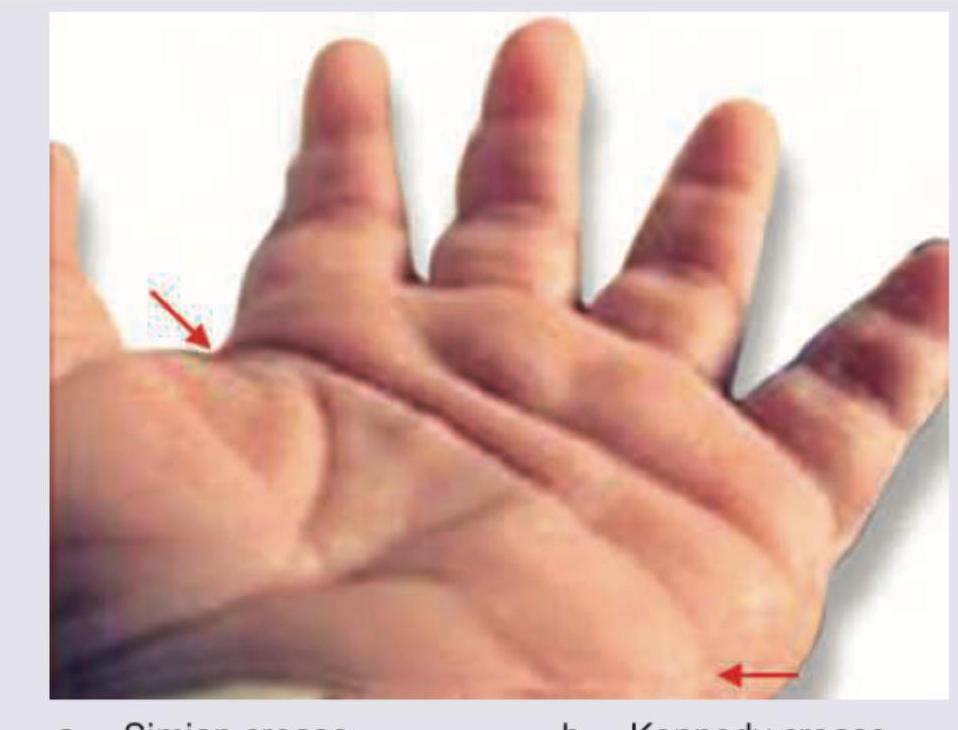
During evaluation of a child with Down syndrome, the following finding is noted. Identify?
Amount of ORS to be given in the first 4 hours to a child with some dehydration is
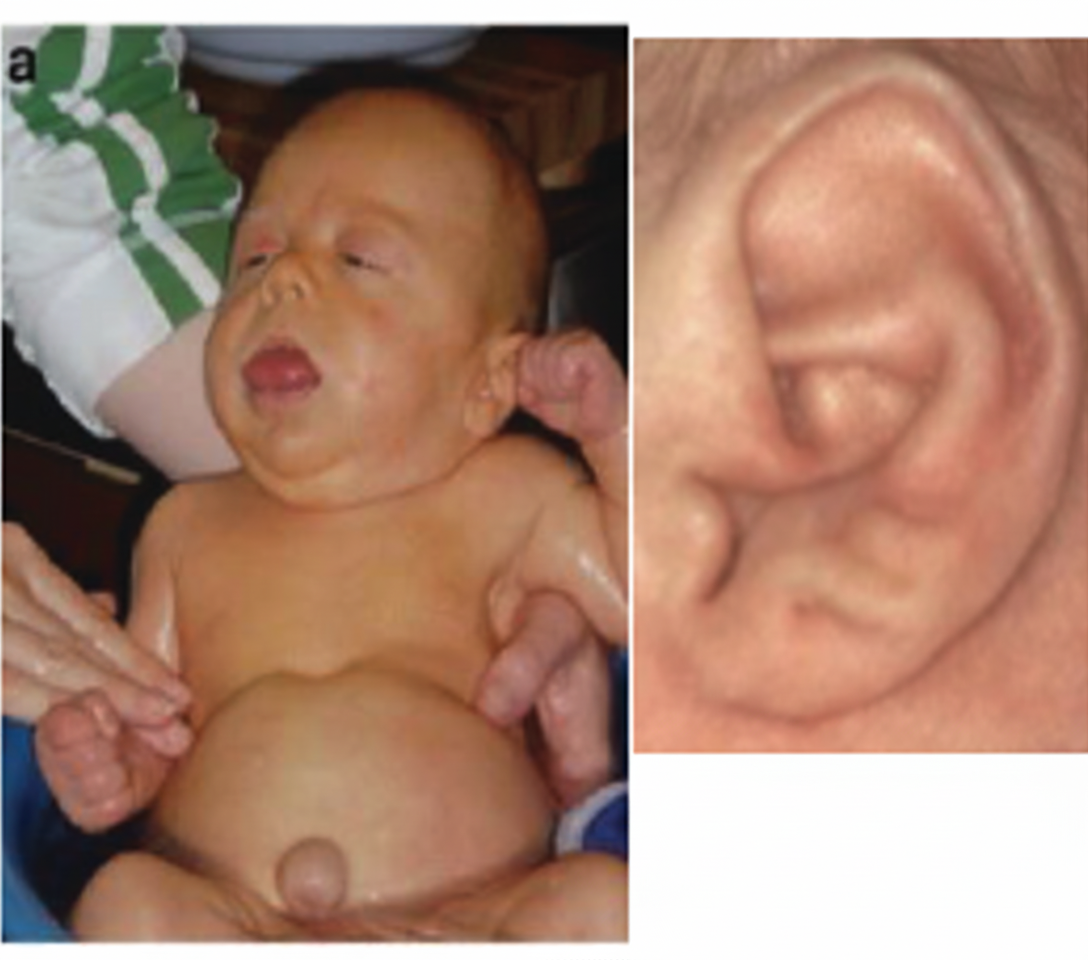
Ear lobe creases in a child are commonly associated with which disorder that also presents with macroglossia and macrosomia?
A 5-year-old short stature child is brought for evaluation. Which disease is the most likely diagnosis as depicted by these pictures of the child, foot and retina?

A sick intubated neonate is having bilateral jerk of both right and left upper limbs with some occasional twitching of neck as well. Likely type of seizures:
Hepatitis B vaccine administered at birth is
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app