
Developmental and Behavioral Pediatrics — MCQs

On this page
Comment on the diagnosis of this child with hypoactive deep tendon reflexes and reduced range of movement at all joints:

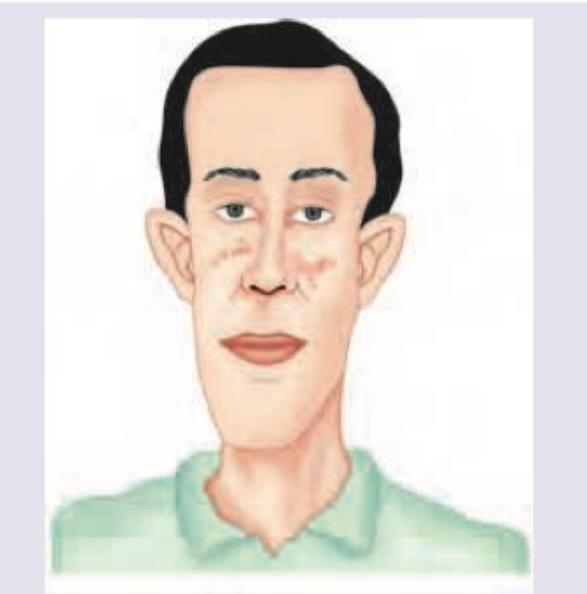
A child presents with characteristic facial features including a long face, prominent forehead, large ears, and prominent jaw. This disorder is also associated with intellectual disability, autistic behavior, and macroorchidism. Which syndrome is being described?
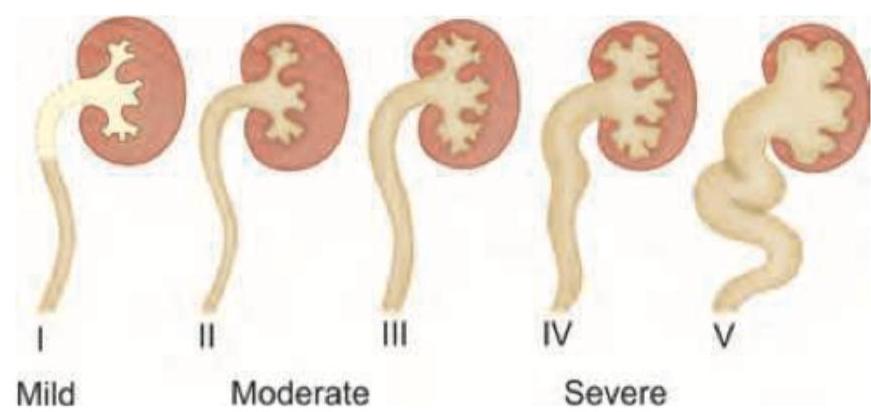
A 2-year-old child presents with developmental delay and hypotonia. The following image shows:

During evaluation of intellectual disability, characteristic facies of the child as below is noted. There is a family history of intellectual disability also. What is the probable diagnosis?
A child presents with complaints of bed wetting. What is the first line of treatment?
What are the reading and writing skills of a child with moderate intellectual disability?
A two year old girl child is brought to the out patient with features of hand wringing stereotype movements, impaired language and communication development, breath holding spells, poor social skills and deceleration of head growth after 6 months of age. The most likely diagnosis is –
All are used in the treatment of nocturnal enuresis except?
True regarding breath holding spells are all EXCEPT:
Nocturnal enuresis should be investigated and treated after:
Practice by Chapter
Normal Development and Variations
Practice Questions
Developmental Delay and Intellectual Disability
Practice Questions
Autism Spectrum Disorders
Practice Questions
Attention Deficit Hyperactivity Disorder
Practice Questions
Learning Disabilities
Practice Questions
Language and Speech Disorders
Practice Questions
Motor Disorders
Practice Questions
Behavioral Problems in Young Children
Practice Questions
Sleep Disorders
Practice Questions
Mood and Anxiety Disorders
Practice Questions
Psychosomatic Disorders
Practice Questions
Developmental Surveillance and Screening
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app