
Systemic Hypertension — MCQs

Which of the following is not a measure of primary prevention of hypertension?
Which of the following is caused by congenital 17 hydroxylase deficiency:
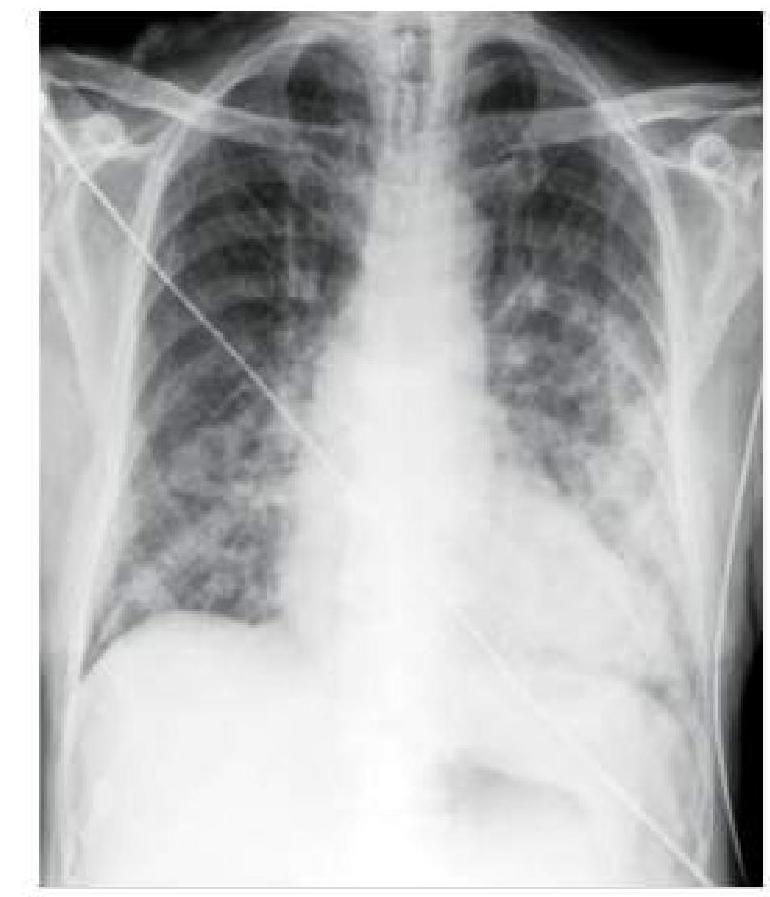
A hypertensive patient who is non-compliant with medication presents to you with sudden onset breathlessness. A chest x-ray was done, which is shown below. How will you manage this patient?
Most common cause of persistent hypertension in a child with intrinsic renal disease is -
A dense persistent nephrogram may be seen in all of the following except:
A 10 year old boy presents to the pediatric emergency unit with seizures. Blood pressure in the upper extremity is measured as 200/140 mm Hg. Femoral pulses were not palpable. The most likely diagnosis is:
An infant presents with LVH and pulmonary complications. ECG shows left axis deviation. The most likely diagnosis is:
A child presented with headache, dizziness, intermittent claudication with occasional dyspnea. The most probable diagnosis is:
A 50-year-old drug abuser presents with fever and weight loss. Exam shows hypeension, nodular skin rash, and peripheral neuropathy. ESR is 100 mm/L, and RBC casts are seen on urinalysis. The most likely condition is:
Child with PDA will NOT have:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app