
Cardiology — MCQs

On this page
The overall heart size in tetralogy of Fallot is usually:
A child has Transposition of the Great Arteries. What maternal condition should be investigated?
Which of the following statements is false regarding Atrial Septal Defect?
A 8-month-old infant presents with severe dyspnea on exertion, clubbing of digits, and bluish sclera. What is the most likely diagnosis based on these findings?
Which one of the following is the most common cause of cyanotic heart disease?
Which type of Atrial Septal Defect (ASD) is most common?
A 3-year-old child presented with a 15-day history of high-grade fever, polymorphous exanthem, rhinorrhea, vomiting, diarrhea, and abdominal pain. On examination, bilateral conjunctival injection with limbal sparing, erythema of oral and pharyngeal mucosa, edema of hands and feet, and mild cervical lymphadenopathy at III and IV levels were noted. Laboratory findings included leucocytosis with neutrophilia and immature forms, elevated erythrocyte sedimentation rate, elevated C-reactive protein, anemia, abnormal plasma lipids, hypoalbuminemia, and hyponatremia. Coronary angiogram findings are also available. What is the most important next step in the management of this child?
Which of the following statements regarding Atrial Septal Defect (ASD) is true?
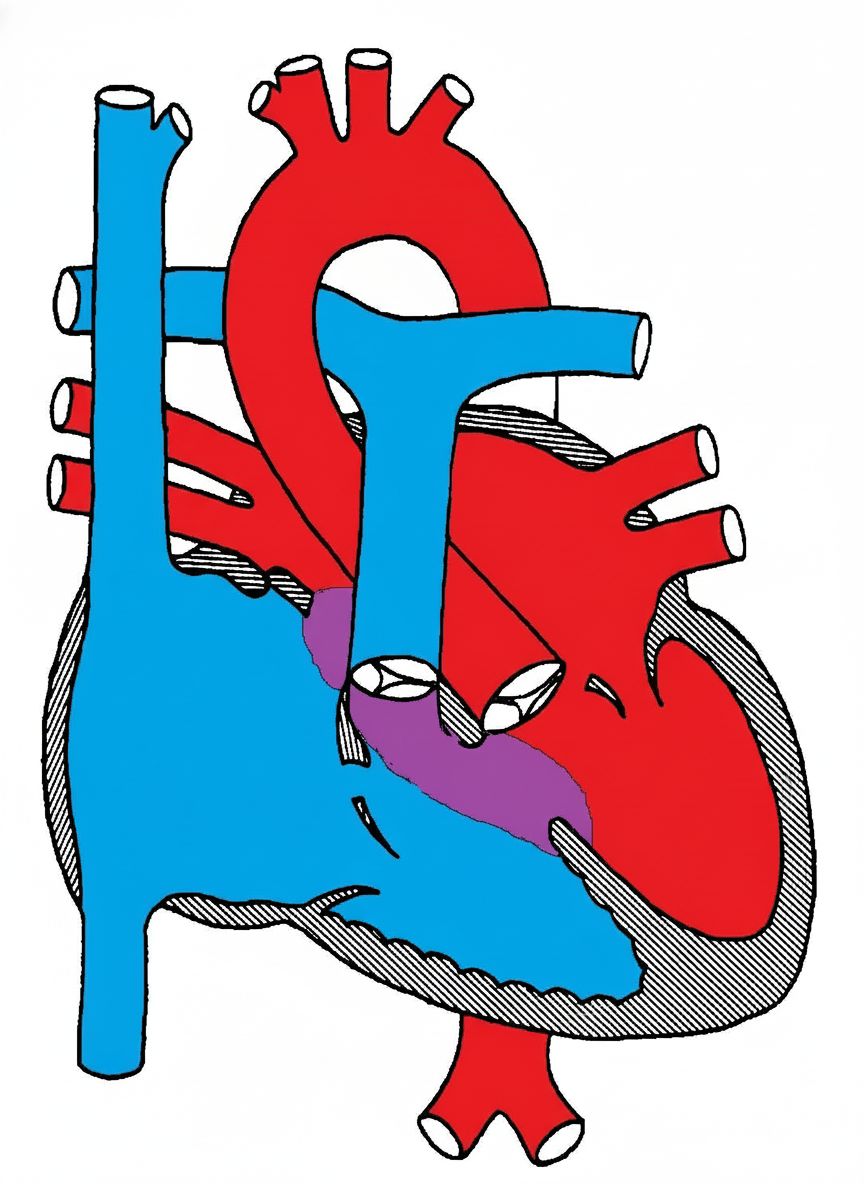
Which congenital heart disease is associated with the defect shown in the diagram below?
Which of the following is NOT a sign of congestive cardiac failure in infants?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app