
Cardiology — MCQs

On this page
Which among the following diagnostic criteria is most characteristic of Kawasaki disease?
What is the most characteristic auscultatory location for a patent ductus arteriosus (PDA) murmur?
In which of the following conditions is an atrial septal defect (ASD) commonly observed?
A child presenting to the clinic with features of Down syndrome. What is the most common cardiac lesion in children with Down syndrome?
Which of the following vasculitides is predominantly seen in children?
Which of the following is the most common cause of syncope in children?
Which of the following congenital heart defects is least likely to cause recurrent pulmonary infections?
A five-day-old, full-term male infant who was severely cyanotic at birth, showed improvement in oxygenation after initial administration of prostaglandin E1 and subsequent balloon atrial septostomy, is most likely diagnosed with which of the following conditions?
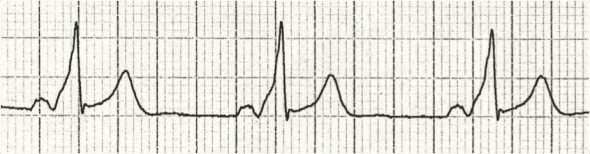
A 4-year-old girl is brought to the pediatrician's office, where her father reports that she suddenly became pale and stopped running while playfully chasing her and her pet Chihuahua. After 30 minutes, she was no longer pale and wanted to resume the game. She has never had a previous episode and has never been cyanotic. Her physical examination was normal, as were her chest x-ray and echocardiogram. An ECG shows a specific pattern indicating which of the following?
What is the most common atrial septal defect in Down syndrome?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app