
Cardiology — MCQs

On this page
In septum primum type of ASD overburden occurs in which chamber?
A 29-day-old child presents with features of congestive cardiac failure and left ventricular hypertrophy. Auscultation shows a short systolic murmur. The most likely diagnosis is:
A child presents with LVH and pulmonary complications. ECG shows left axis deviation. Most likely diagnosis is:
An 8-month-old female child presented to the emergency department with a heart rate of 220/minute and features of congestive heart failure. Her heart rate returned to normal after administering intravenous adenosine. What is the most likely diagnosis?
The heart lesion not found in Congenital Rubella infection is –
Which of the following does not complicate into CHF –
A child presented with headache, dizziness, intermittent claudication with occasional dyspnea. The most probable diagnosis is:
True statement about Rheumatic fever in children -
Uncommon finding in congestive cardiac failure in a newborn -
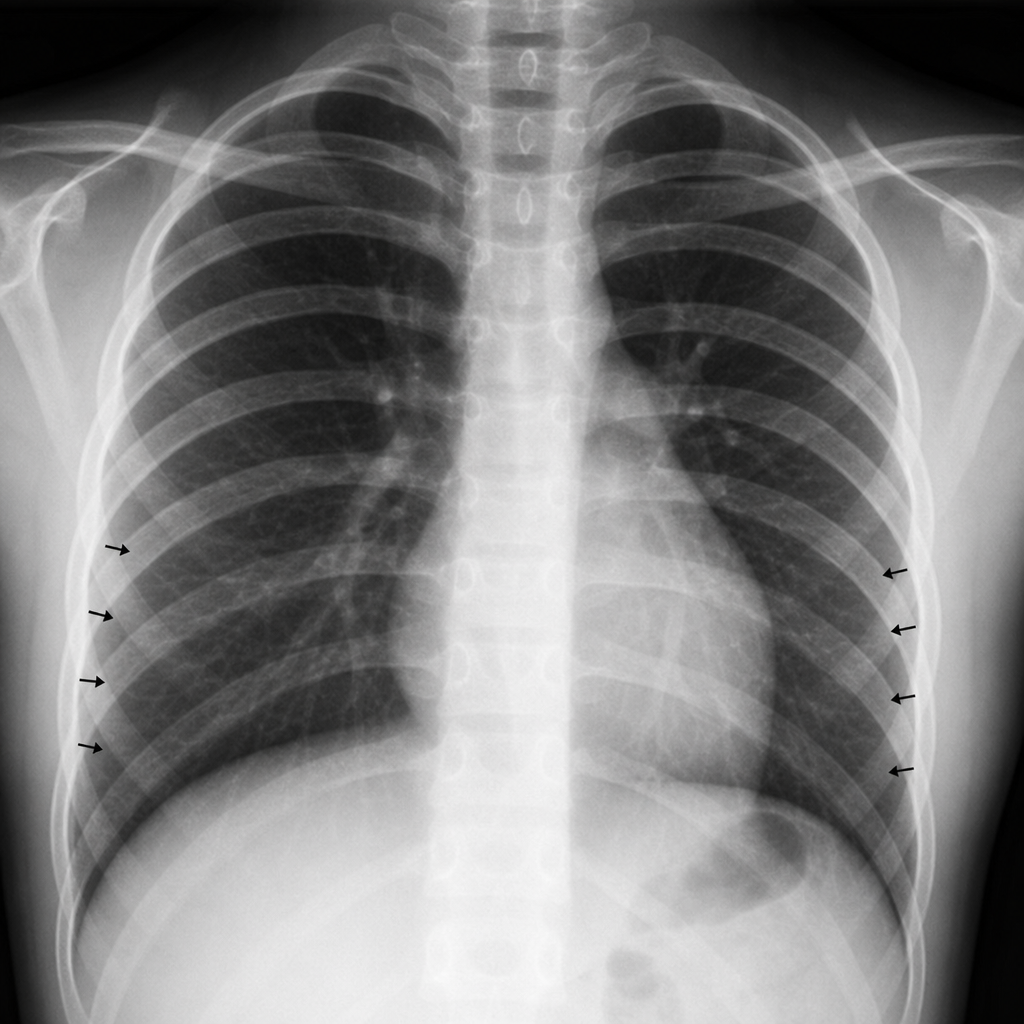
A 41/2- year-old girl always had to wear warm socks even is summer season. On physical examination, it was noticed that she had high blood pressure and her femoral pulse was weak as compared to radial and carotid pulse. a chest radiograph showed remarkable notching of ribs along with their lower borders. This was due to -
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app