
Cardiology — MCQs

On this page
A 9 year old boy with Fallot's tetralogy, had high grade fever followed by focal seizure 2 days prior to hospital admission. His blood counts were increased and predominantly polymorphs. CT scan of the head showed a focal lesion suggestive of an abscess. Where would be the commonest location of brain abscess in this patient?
Congenital cyanotic heart disease with pulmonary oligemia is seen with –
Which of the following is least likely in PDA?
A child after 4 weeks of age presents with an acyanotic ejection systolic murmur. Which of the following is the most likely cause?
Tetralogy of Fallot is characterized by following except –
A mother brings her 5-year-old boy to see you as a General Physician. On examination, he has red eyes, dry, cracked lips and a rash on his hands and feet. He also has cervical lymphadenopathy. What is the most important investigation to rule out a serious complication of this condition?
Commonly associated in tetralogy of Fallot is:
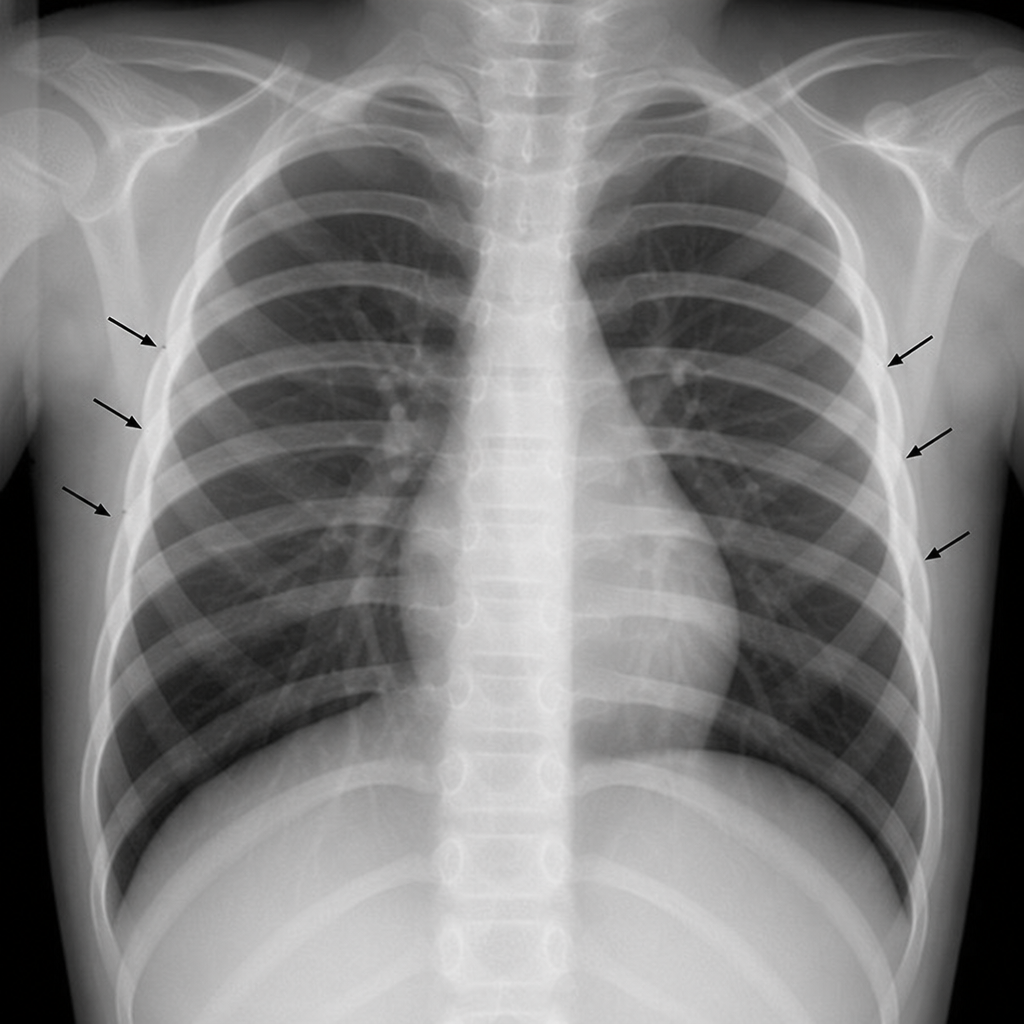
A 4 1/2- year-old girl always had to wear warm socks even is summer season. On physical examination, it was noticed that she had high blood pressure and her femoral pulse was weak as compared to radial and carotid pulse, a chest radiograph showed remarkable notching of ribs along with their lower borders. This was due to:
Most common cardiac defect seen in Rubella syndrome
The most common paediatric cardiac tumour among the following is
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app