
Cardiology — MCQs

On this page
The following cardiac defects are characterized by ductus dependent blood flow except –
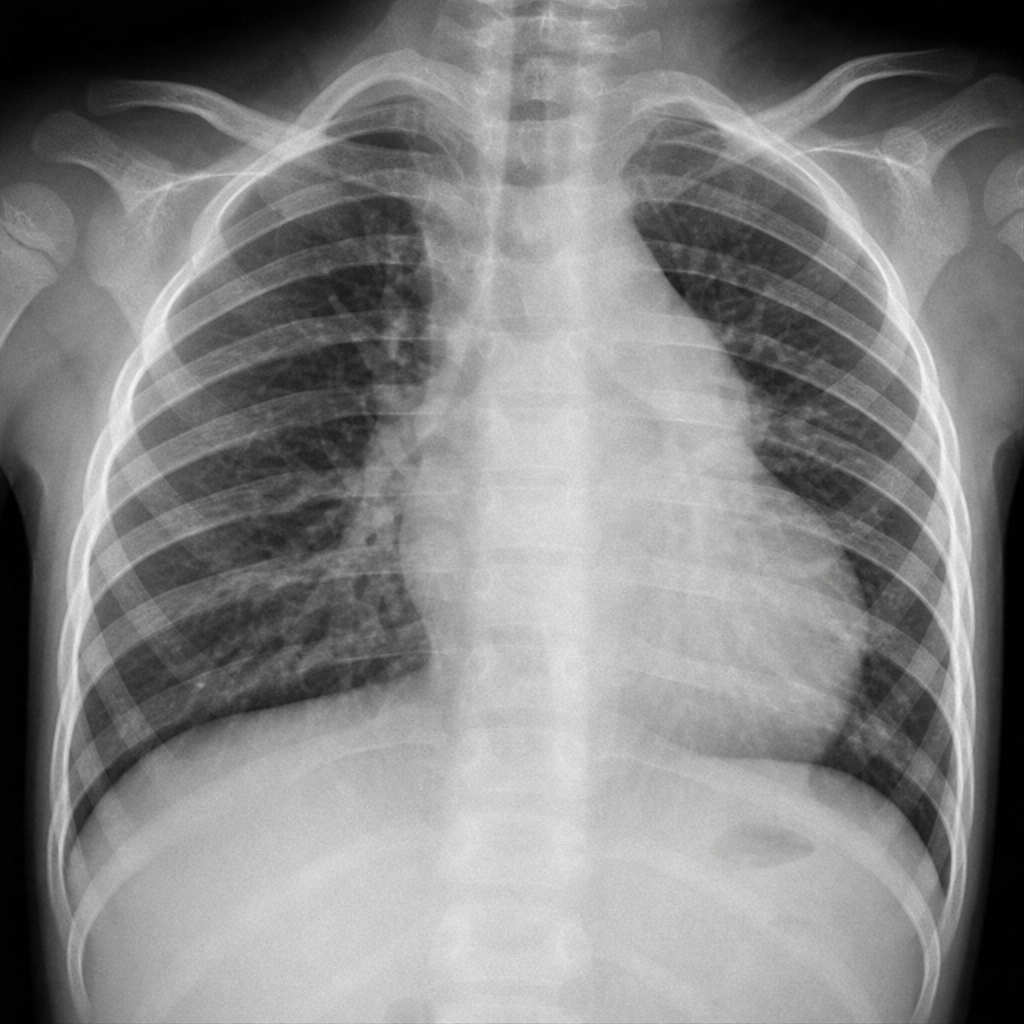
A child comes with cyanotic spells and chest X-ray was as shown below; What is the most probable diagnosis?
A five-year-old girl presents with fever and conjunctivitis. Physical examination is significant for oral erythema and fissuring along with a generalized maculopapular rash and cervical lymphadenopathy. What is the most likely diagnosis?
Most common cardiac anomaly in Turner syndrome: CMC (Vellore) 07; CMC (Ludhiana) 13; UPSC 14
PDA true is all except -
A 2-month-old infant is brought to the clinic because of poor feeding, sweating, and difficulty breathing. The parents state that she was doing very well, and has actually been a "very easy going baby", until about a week ago. They assumed that she was developing a "cold", but it has not passed, and the symptoms have been worsening. Cardiac examination reveals a loud, harsh systolic murmur with a thrill that is heard best at the left sternal border. The most likely underlying abnormality is
Which of the following is the most common type of congenital cardiac cyanotic anomaly?
A 2-week-old baby is irritable and feeding poorly. On physical examination, the infant is irritable, diaphoretic, tachypneic and tachycardic. There is circumoral cyanosis, which is not alleviated by nasal oxygen. A systolic thrill and holosystolic murmur are heard along the left sternal border. An echocardiogram reveals a heart defect in which a single arterial trunk overrides a ventricular septal defect. What is the appropriate diagnosis?
True about VSD are all except -
Which of the following congenital heart diseases is MOST OFTEN associated with decreased pulmonary blood flow?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app