
Cardiology — MCQs

On this page
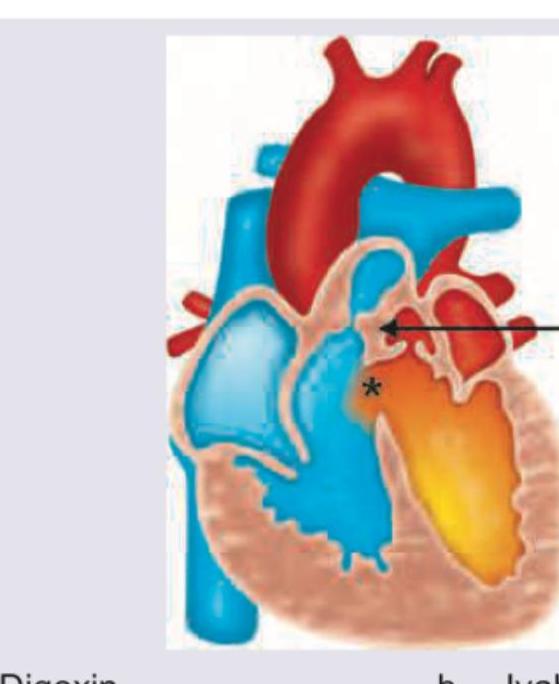
A neonate presents with a congenital heart disease as shown below. Which drug should be started immediately? (Recent NEET Pattern 2016-17)
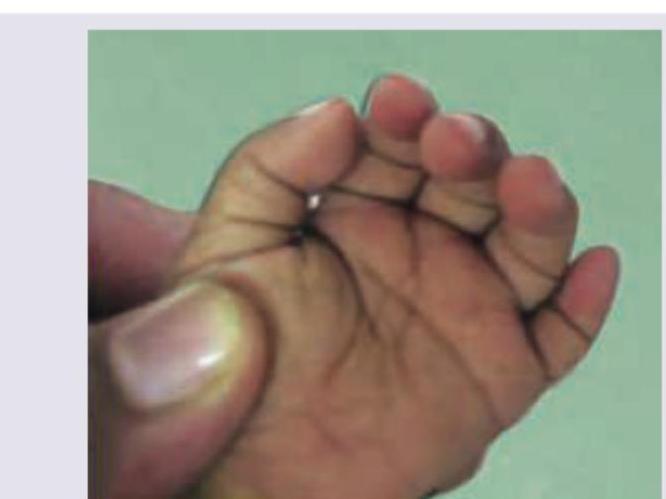
A child with Down syndrome presents with the finding shown. Which congenital heart disease is most commonly associated with this condition?
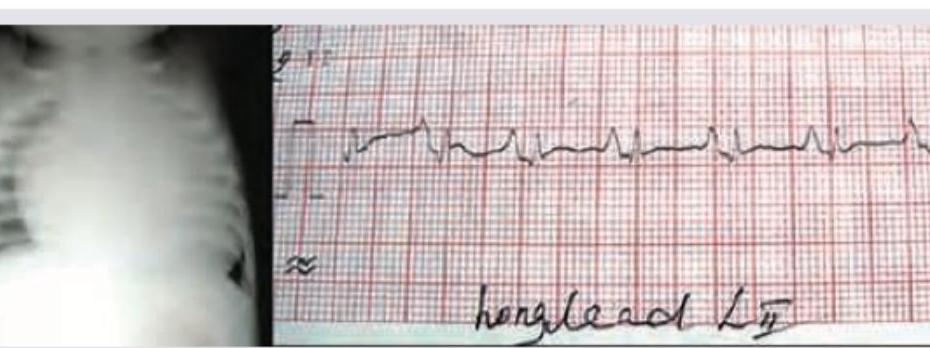
A 1 day old neonate presents with central cyanosis. CXR and ECG are performed (shown in the image). Which diagnosis is most consistent with these findings?
A 4-year-old boy presents with 6 days of fever, bilateral non-exudative conjunctival injection, strawberry tongue with cracked lips, erythema and edema of the hands and feet, and a polymorphous truncal rash. The images below show key clinical and imaging findings of his diagnosis. Choose the TRUE statement regarding this disease:

Child presents with strawberry tongue, fever for 5 days, cracked lips, Periungual peeling of the skin and bulbar congestion. Which of the following cardiac lesions will be seen in this child?
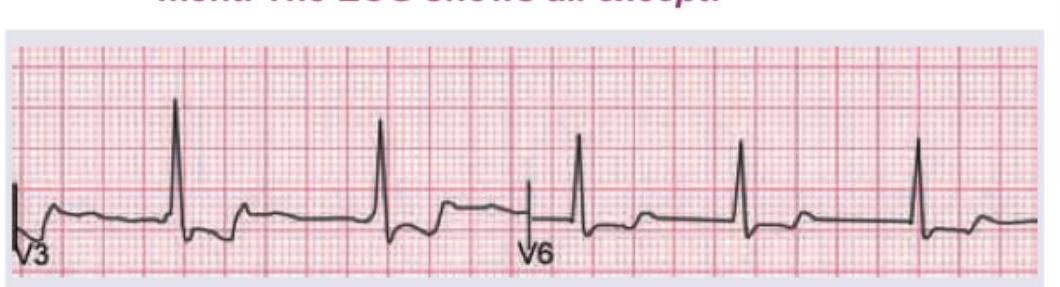
A 1-week-old neonate presents with anoxic spells and single S2. CXR shows all except:

A 3-year-old child presents with persistent fever for 5 days and the clinical features shown in the image. What is the most likely diagnosis?

A 1-year-old child with CHD is on heart failure treatment. The ECG shows all except:
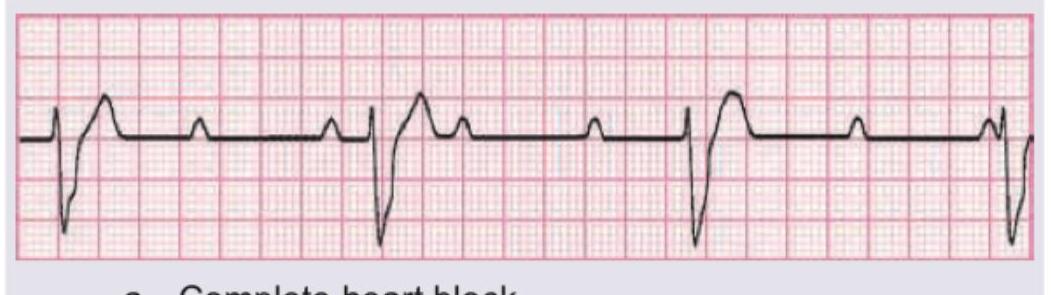
The given ECG of a neonate born to a mother with SLE shows?
Which one of the following is a cyanotic congenital heart disease?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app