
Cardiology — MCQs

On this page
Which one of the following congenital heart diseases presents with cyanosis without cardiomegaly and/or congestive heart failure?
In a 5-year-old child, instead of the physiological splitting of the second heart sound (S2), which is expected only during inspiration, a wide and fixed split of S2 is heard during both inspiration and expiration. What condition is associated with this finding?
Which cardiac anomaly is associated with Tetralogy of Fallot?
A 5-year-old child presents with exertional dyspnea and a history of cyanotic spells. On examination, there is clubbing and a harsh systolic murmur heard at the left upper sternal border. Chest X-ray is shown below. What is the most likely diagnosis?
A child presents with kawasaki disease with multiple small coronary artery aneurysms. Treatment is?
What could be the possible diagnosis for a newborn exhibiting weak lower limb pulses and strong upper limb pulses?
A 9-month-old infant presents with severe respiratory distress, central cyanosis not improving with oxygen, and a harsh systolic murmur. Chest X-ray shows boot-shaped heart with decreased pulmonary vascular markings. Echocardiography confirms the diagnosis. What is the most likely underlying cardiac defect?
A 4-year-old child presents with high-grade fever for 5 days, bilateral non-purulent conjunctival injection, strawberry tongue, cervical lymphadenopathy (>1.5 cm), and polymorphous rash. On day 6, desquamation of fingertips begins. Echocardiography shows coronary artery dilation. What is the most appropriate immediate treatment?
A 3-year-old child is brought to the clinic with a history of cyanosis since infancy. Which of the following is a component of Tetralogy of Fallot (TOF)?
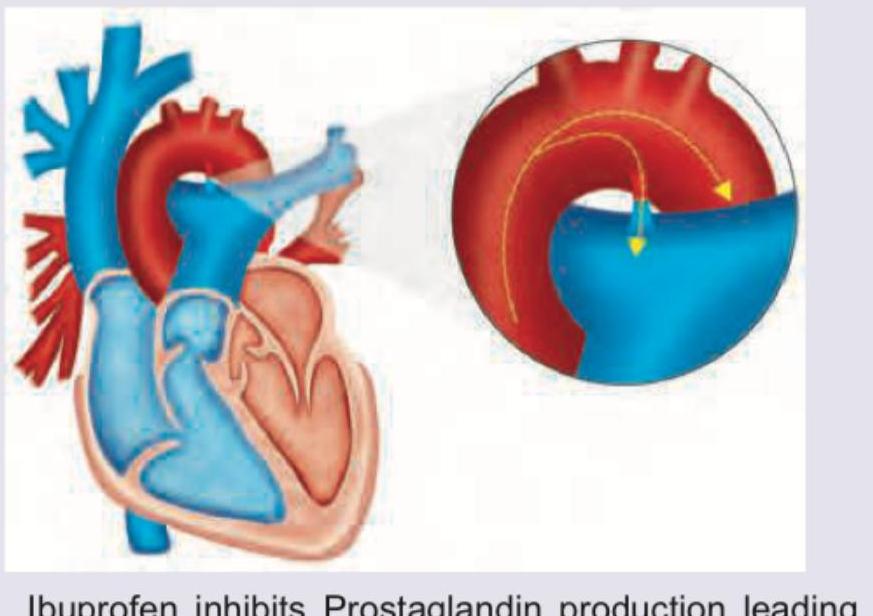
A 6-week-old term baby presents with poor feeding. All are true about the isolated PDA condition shown except:
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app