
Cardiology — MCQs

On this page
A child presents with failure to thrive. Despite counseling on nutritional improvement, the parents report no change. What is the likely diagnosis?
All of the following conditions are associated with a systolic thrill in the left 2nd and 3rd intercostal space, EXCEPT:
All of the following statements about Kawasaki disease are true, EXCEPT:
Which of the following is a true statement about Coarctation of the Aorta?
A newborn presents with deepening cyanosis at birth, with congestive heart failure and a normal first heart sound. X-ray reveals cardiomegaly. What is the diagnosis?
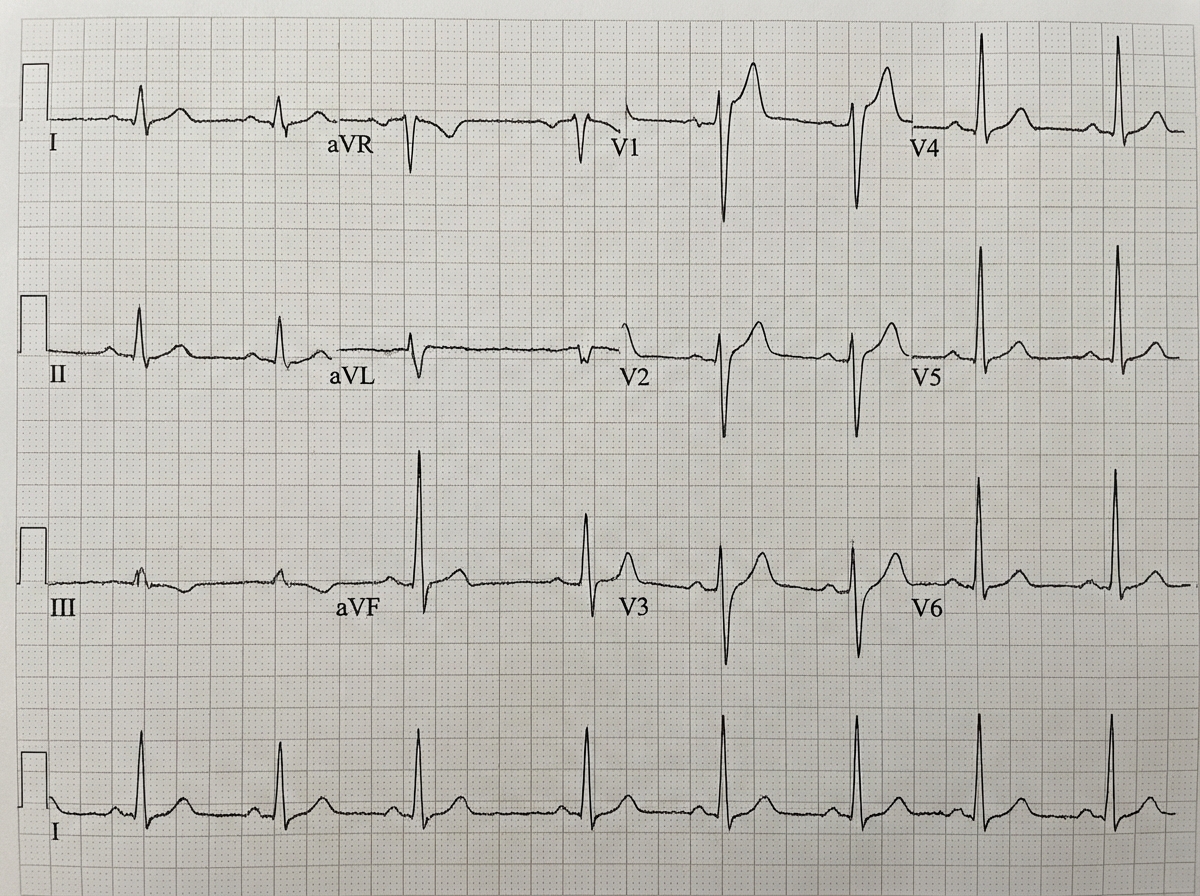
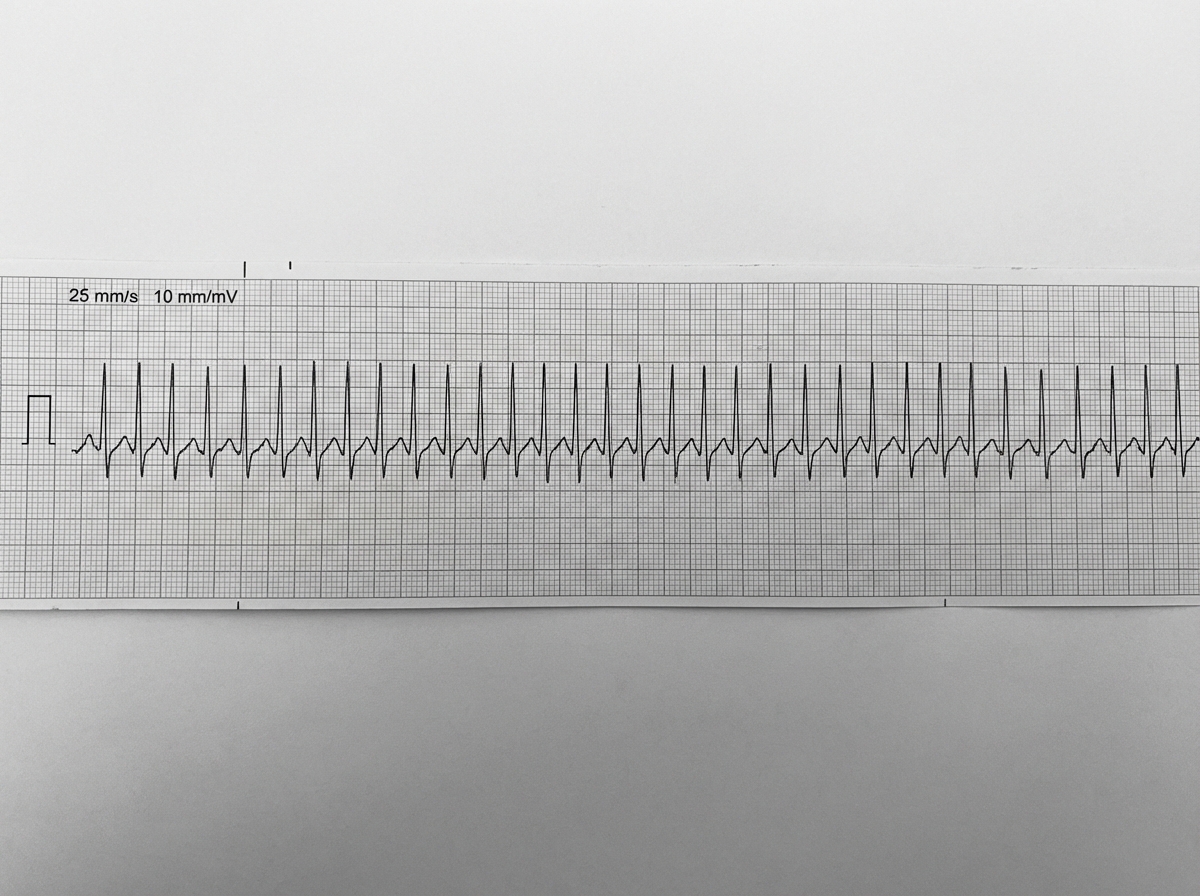
A 5-month-old pale and lethargic male infant presents to the emergency department. On examination, heart rate is 240 bpm and does not change with crying. Lungs are clear and there is no hepatomegaly. An ECG is provided. Which of the following is the first step in the management of this patient?
A severely ill 3-year-old child presents with fever, enlarged cervical lymph nodes, and a desquamating rash involving the palms, soles, and mouth. What complication should be monitored for in this child?
Noonan syndrome is characterized by all of the following EXCEPT:
Intravenous immunoglobulin is indicated in which of the following conditions?
Which of the following is NOT a feature of Holt-Oram Syndrome?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app