
Cardiology — MCQs

On this page
In a 12-year-old boy, which of the following is the best statement regarding aortic valve stenosis?
Turner syndrome is associated with which of the following?
In a 5-year-old child, instead of the physiological splitting of the second heart sound (S2) which is expected only during inspiration, a wide and fixed split of S2 is heard during both inspiration and expiration. A wide fixed split of the second heart sound can be seen in all of the following EXCEPT?
Which NSAID is most commonly used in Rheumatic fever?
A 4-year-old child presents with high fever, a toxic appearance, eruptions on the trunk and proximal extremities, bilateral bulbar conjunctivitis without discharge, fissured-crusted red lips, and limb edema making walking difficult. She also has desquamation in the perineum and fingertips, along with cervical adenopathy. What is the most likely diagnosis?
A 3-month-old infant is diagnosed with a deletion at the 22q11 chromosome. A routine cardiovascular examination reveals severe congenital cardiac malformation. Which of the following malformations will most likely be associated with 22q11 syndrome?
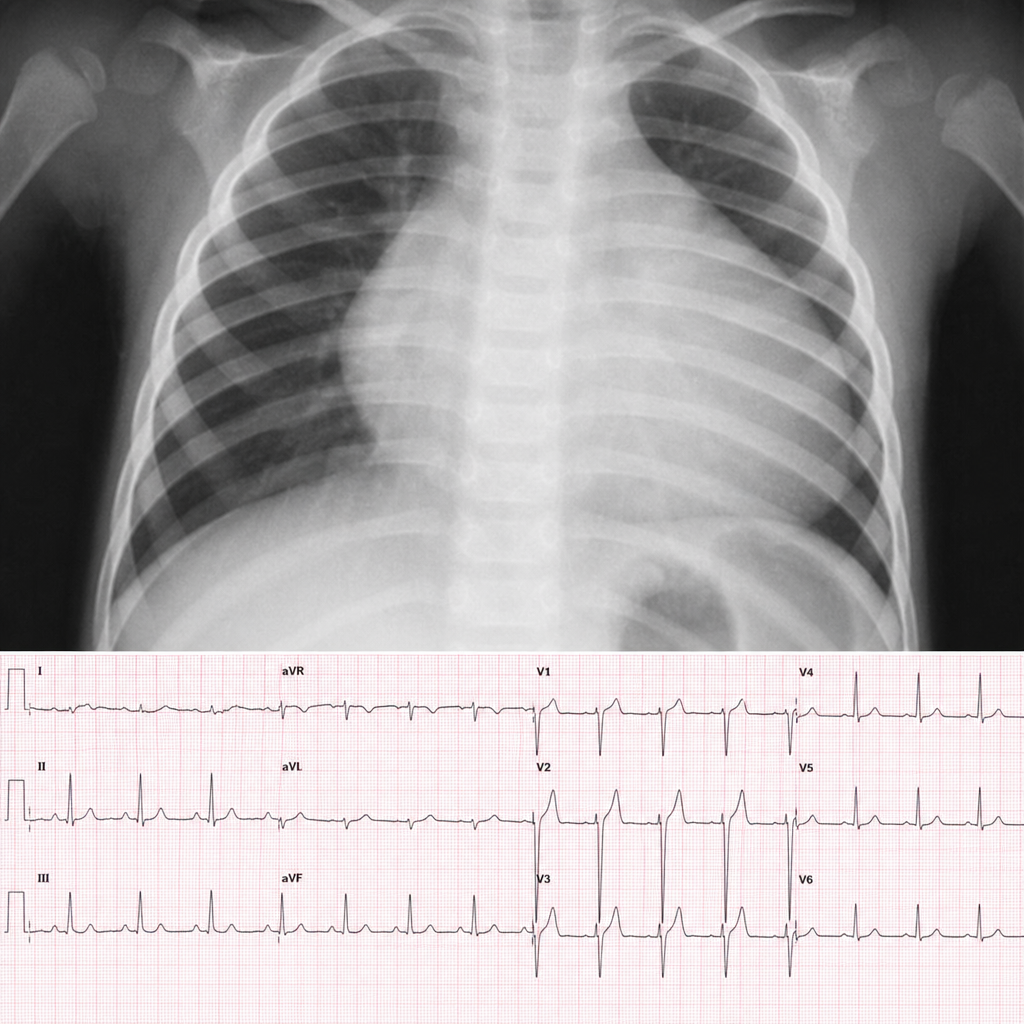
A 2-month-old baby with central cyanosis presented with specific findings on chest X-ray and ECG. What is the most probable underlying diagnosis?
What is the most common heart abnormality in children?
According to the American Heart Association & World Heart Federation 2015 criteria, low risk for acute rheumatic fever is defined as an incidence of less than which of the following per 100,000 school-aged children per year?
Which of the following is NOT a component of Kawasaki disease?
Practice by Chapter
Congenital Heart Diseases: Cyanotic
Practice Questions
Congenital Heart Diseases: Acyanotic
Practice Questions
Rheumatic Heart Disease
Practice Questions
Kawasaki Disease
Practice Questions
Infective Endocarditis
Practice Questions
Myocarditis and Cardiomyopathies
Practice Questions
Arrhythmias in Children
Practice Questions
Heart Failure in Children
Practice Questions
Pulmonary Hypertension
Practice Questions
Systemic Hypertension
Practice Questions
Dyslipidemia in Children
Practice Questions
Cardiac Evaluation and Diagnostics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app