
Adolescent Sexuality — MCQs

Transmission assessment survey (TAS) is done for which of the following purposes?
A male with hyperpigmentation tanner stage 5 presents with hypertension & precocious puberty. The causative defect is:
A 25-year-old woman presents with vaginal discharge and vulvovaginal irritation. Wet mount shows motile trichomonads. She mentions having a similar infection 2 months ago treated with single-dose metronidazole. What is the most likely explanation for her current infection?
The contraceptive which is contraindicated in DVT is?
Which of the following is not a long-acting reversible contraceptive method?
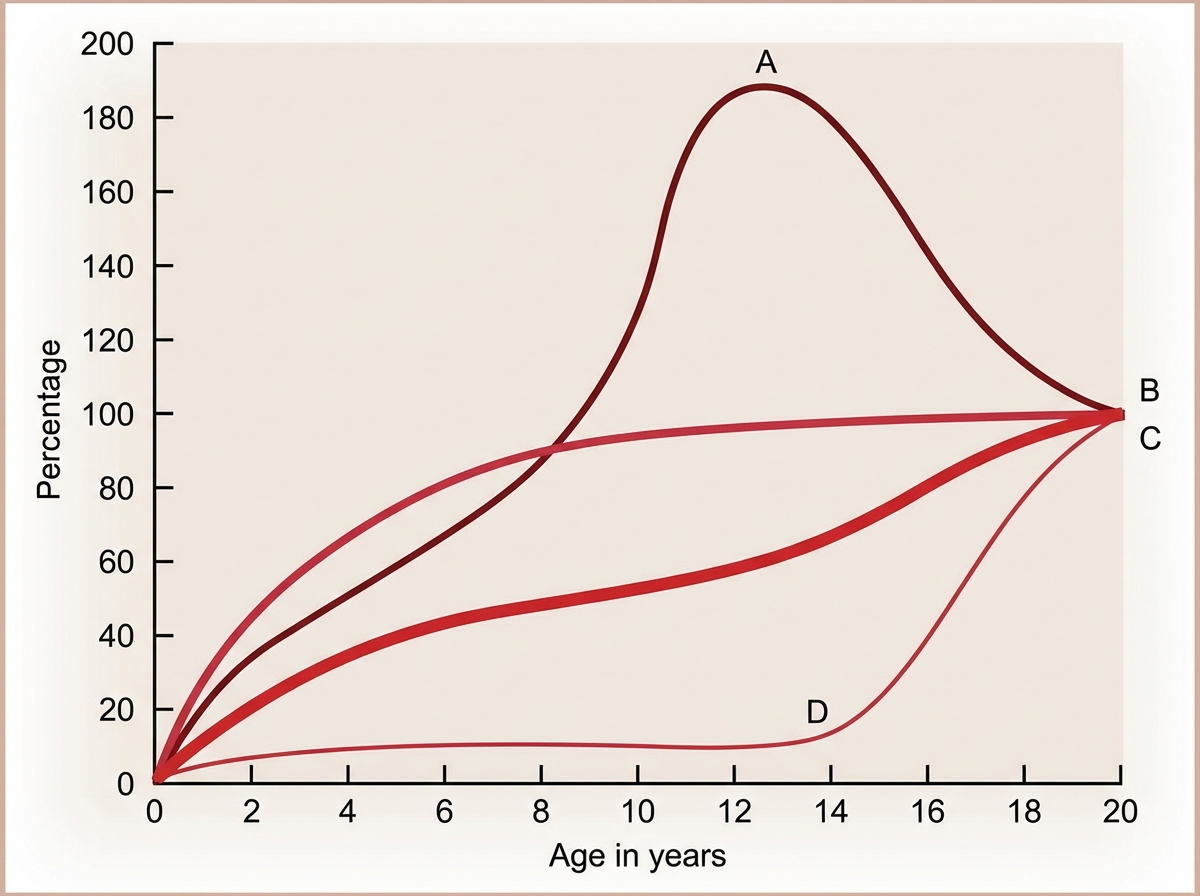
The Image shows the growth curve of different organs with age. Identify A in the graph.
A 14-year-old victim of sexual assault with 22 weeks gestation has been brought for Medical Termination of Pregnancy (MTP). Which of the following statements is true?
A sexually active 16-year-old presents for STI screening with recent assault history, multiple partners, inconsistent condom use. Which comprehensive prevention strategy is most appropriate?
What is the preferred method of contraception for a female with a family history of ovarian cancer?
What is the age range of adolescence?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app