
Vascular Pathology — MCQs

On this page
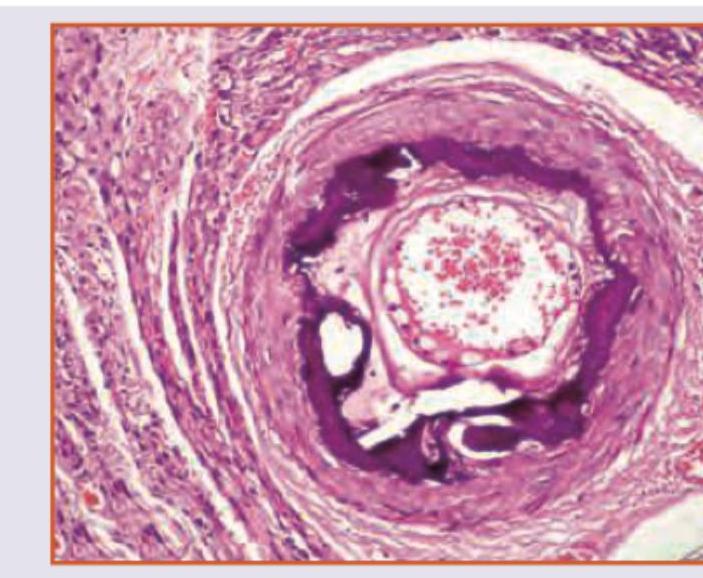
Which is true about the image shown?
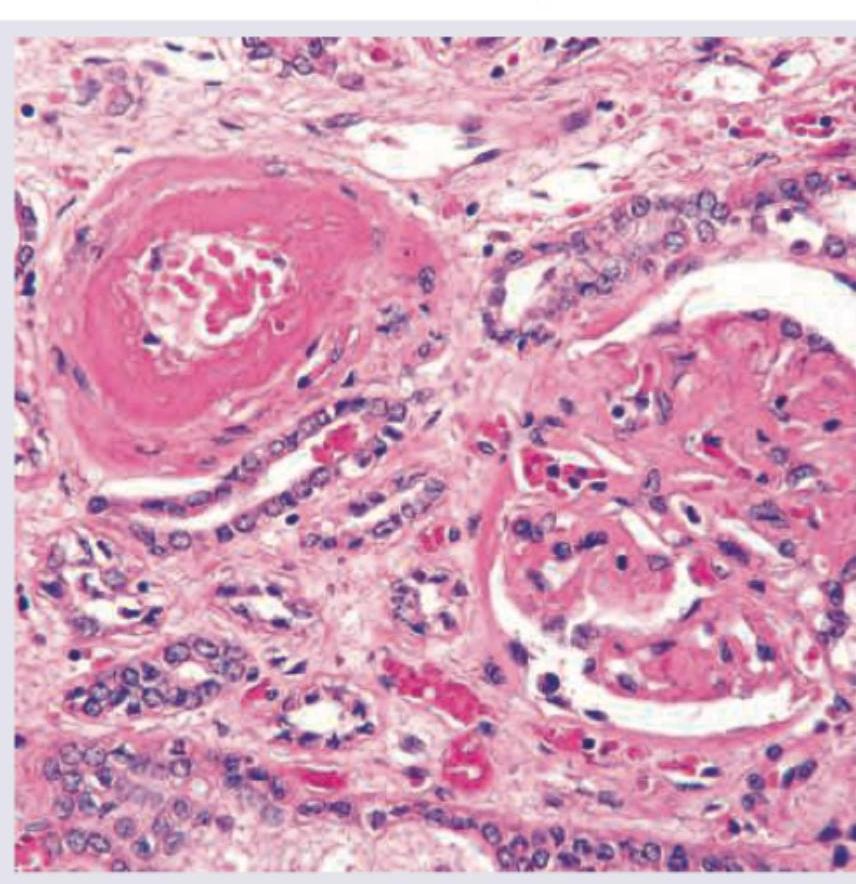
A 45-year-old male with severe hypertension presents with acute renal failure. A renal biopsy shows the histopathological findings in the image. What is the most likely diagnosis?
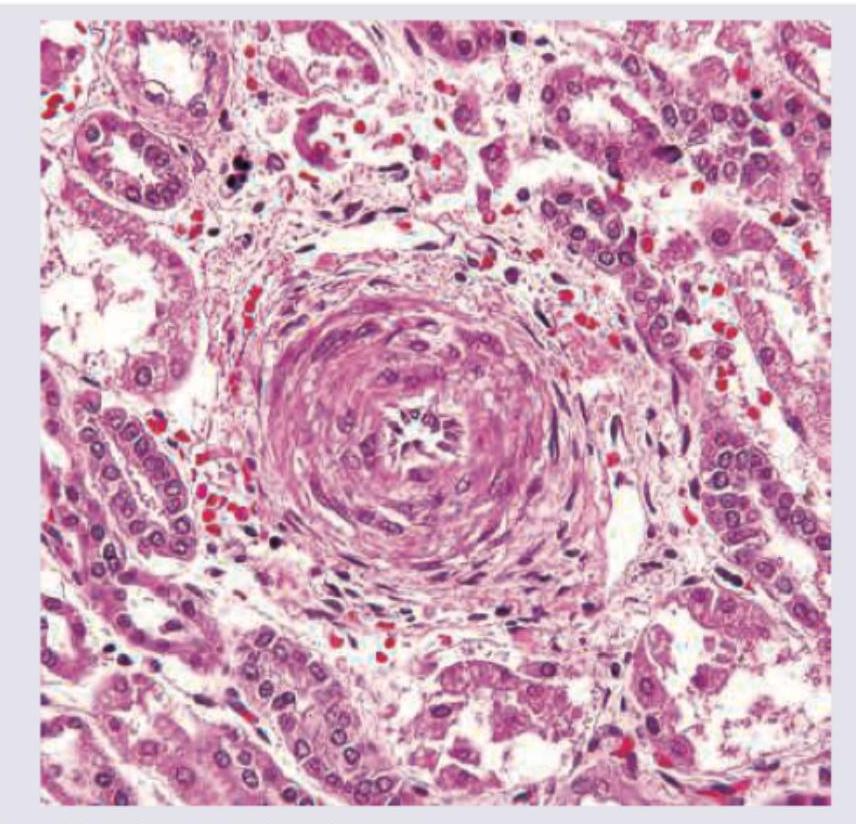
The histological image shows a blood vessel with characteristic changes. What is the most likely diagnosis?
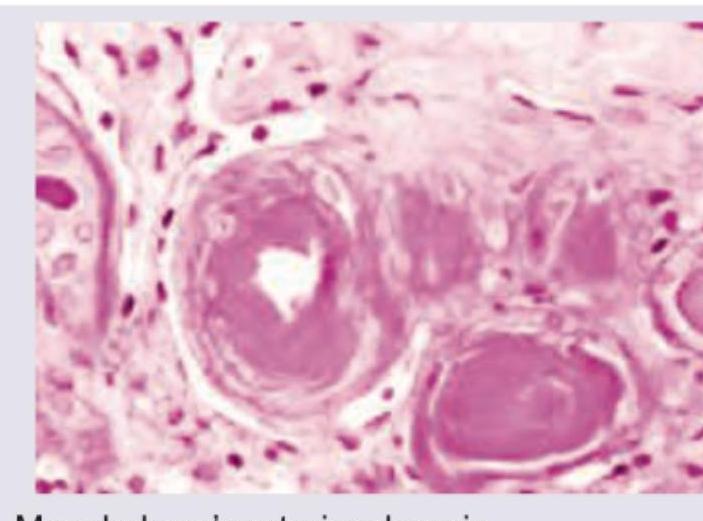
Which is true about the image shown?
Virchow's triad includes all except:-
Berry aneurysm most commonly occurs due to?
Angiofibroma bleeds profusely because:
In polyarteritis nodosa, aneurysms are seen in all organs EXCEPT:
True about Henoch-Schonlein purpura are the following, EXCEPT:
White infarct is not seen in which of the following
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app