
Vascular Pathology — MCQs

On this page
What is the earliest lesion observed in atherosclerosis?
A 70-year-old man presents with abdominal pain and an abdominal mass. Angiography reveals an aneurysm of the abdominal aorta. What is the most likely cause?
A 40-year-old man presents with a 2-week history of recurrent oral ulcers, genital ulcers, intermittent arthritic pain of the knees, and abdominal pain. Physical examination reveals shallow ulcerations of the mucosa of the glans penis, as well as oral aphthous ulcers and conjunctivitis. Which of the following is the most likely diagnosis?
Magic syndrome is seen in which of the following conditions?
What is the earliest lesion observed in atherosclerosis?
Atherosclerosis initiation by fibroblast plaque is mediated by injury to?
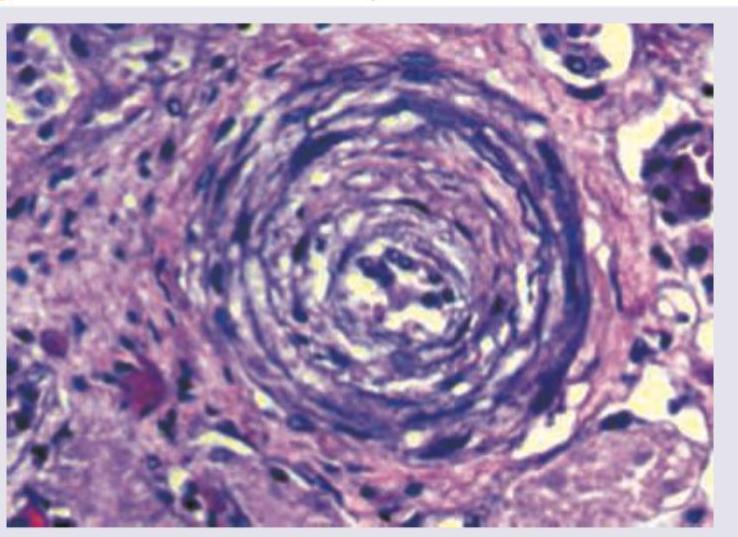
A 62-year-old man presented in the medical emergency with complaints of severe headache and dizziness. His blood pressure was recorded to be 200/146 mm Hg. Pathological slide presentation is given in the image below. What is the most likely diagnosis?
A 50-year-old patient with family history positive for premature coronary artery disease is found to have lumps on Achilles tendon. Biopsy from the lesion shows presence of:
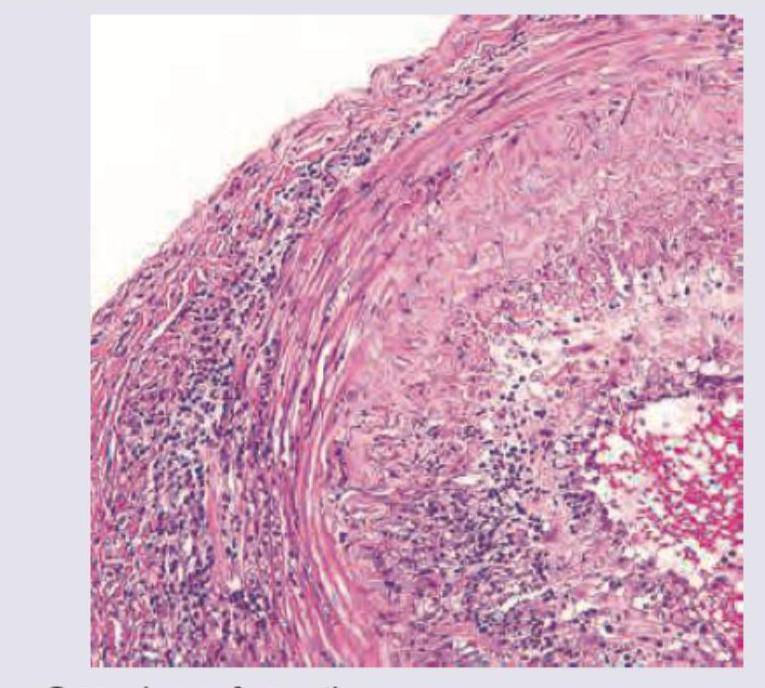
A 70-year-old retired military personnel presents with daily temporal headache and same sided blurring of vision. The Biopsy of Temporal artery was performed. All are true about the condition except:
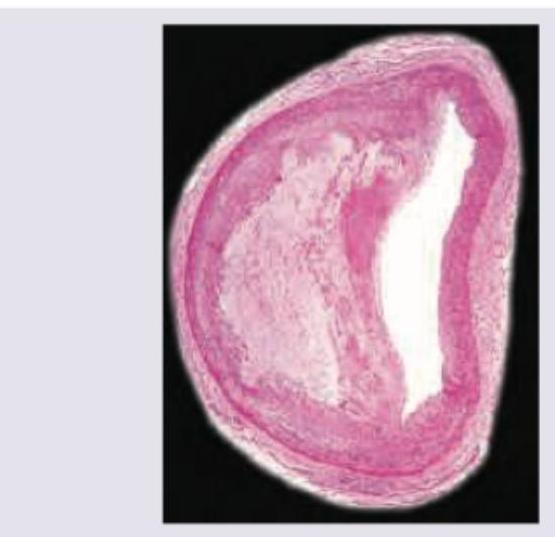
The image shows presence of:
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app