
Vascular Pathology — MCQs

On this page
What is the primary role of scavenger receptors in the development of atherosclerotic plaques?
Which of the following is not a large vessel vasculitis?
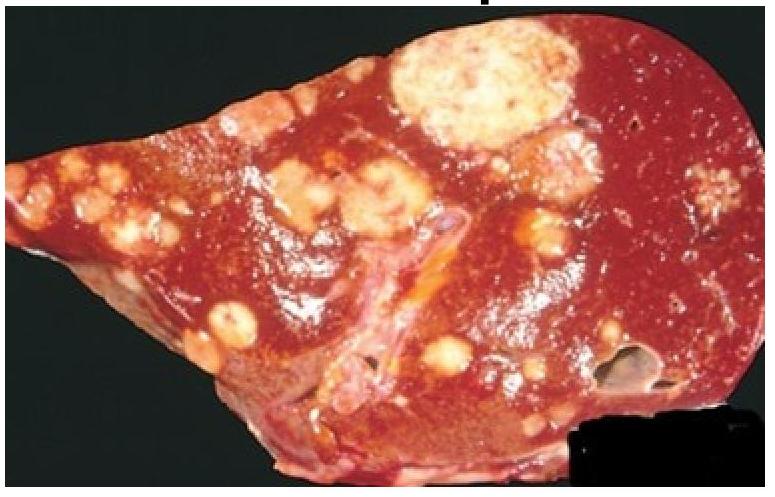
A woman shows symptoms of massive pulmonary thromboembolism. Based on the gross appearance of the liver autopsy, which of the following statements best characterizes the patient’s condition?
The tissue of origin of the Kaposi's sarcoma is
Obliterative endarteritis in vasa vasorum is seen in -
Which type of artery is most commonly involved in PAN?
Which of the following is a type of small vessel vasculitis?
Fibrinoid necrosis with neutrophilic infiltration is seen in ?
All of the following are true regarding fibromuscular dysplasia EXCEPT:
Which HLA antigen is associated with thromboangitis obliterans?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app