
Vascular Pathology — MCQs

On this page
Which is associated with vasculitis of medium sized vessels
In polyarteritis nodosa, aneurysms are seen in all organs EXCEPT:
True about Henoch-Schonlein purpura are the following, EXCEPT:
Which one of the following does not cause small vessel vasculitis?
Which of the following is NOT a large vessel vasculitis?
Which of the following is false about polyarteritis nodosa
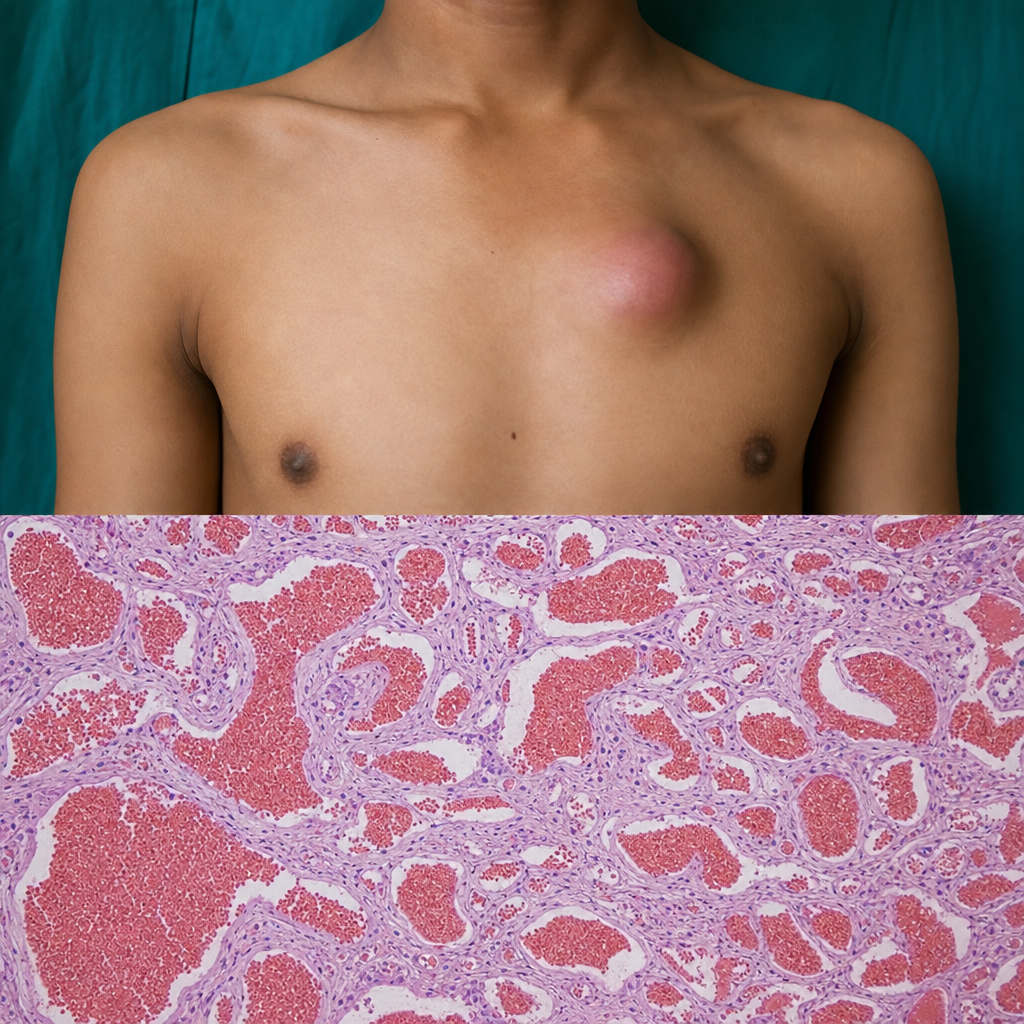
A teenager has a progressively increasing soft reddish swelling on his chest. Its histological appearance is given below. Which of the following is the likely diagnosis?
Most characteristic finding in granulomatosis with polyangiitis?
A 70-year-old woman with a history of hypertension presents with a pulsatile abdominal mass. A CT scan shows an aortic aneurysm. Which histologic finding is most likely to be present in this patient?
A red soft to firm swelling on the sternum shows proliferation of endothelial cells forming vascular channels on biopsy. What is the most likely diagnosis?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app