
Vascular Pathology — MCQs

On this page
All endothelial cells are involved in the production of thrombomodulin EXCEPT those found in:
Which of the following changes does NOT occur in malignant hypertension?
Which of the following is NOT an ANCA-associated vasculitis?
What is the characteristic pathological feature of pyogenic granuloma?
What is the characteristic pathological feature of pyogenic granuloma?
IgA deposits are seen on a skin biopsy in which of the following conditions?
Which of the following does NOT predispose to atherosclerosis?
What is the earliest lesion observed in atherosclerosis?
A 30-year-old AIDS patient presents with complaints as shown below. All are true about the condition except?

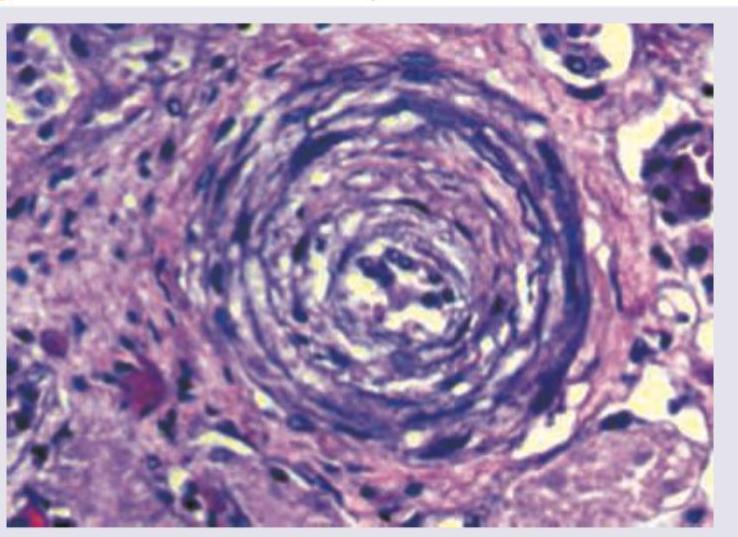
A 62-year-old man presented in the medical emergency with complaints of severe headache and dizziness. His blood pressure was recorded to be 200/146 mm Hg. Pathological slide presentation is given in the image below. What is the most likely diagnosis?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app