
Vascular Pathology — MCQs

On this page
Which of the following is not a recognized etiology of Kaposi sarcoma?
What is the most common cause of aortic aneurysm?
A study of atheromatous plaques shows that the release of growth factors, including PDGF, FGF, and TNF-a, leads to increased extracellular matrix production. As a result, the size of the plaques increases. Which of the following cells is most likely to release these growth factors in the plaques?
Which of the following is NOT a histological feature of Kaposi's sarcoma?
A person with involvement of the upper respiratory tract, lungs, and kidneys shows evidence of granulomas on histopathology. What is the most likely diagnosis?
Atheromatous changes of blood vessels affect which organ earliest?
What is the typical histological change seen in benign hypertension?
Which of the following statements is NOT true regarding hypersensitivity vasculitis?
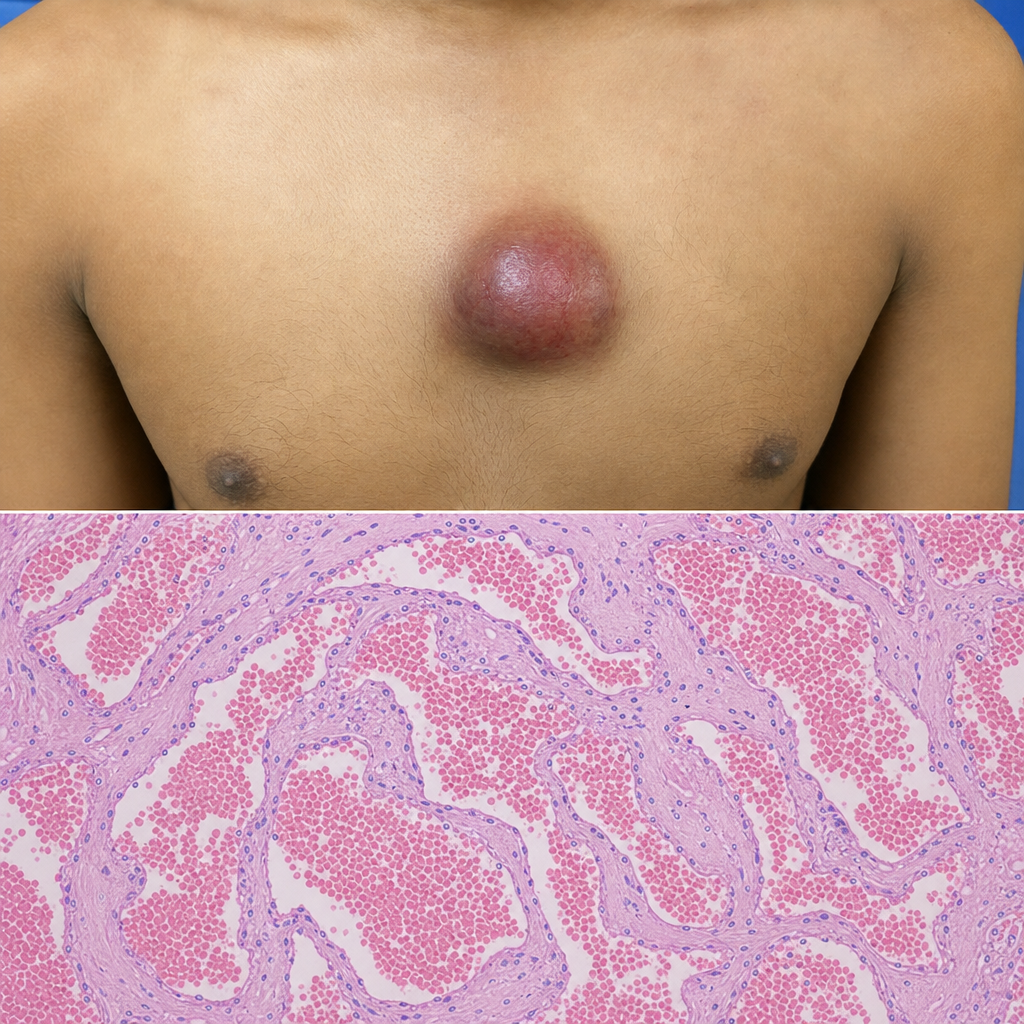
A 20-year-old patient presents with a soft to firm reddish swelling progressing in size over the precordium. Histopathological examination showed findings consistent with this lesion. What is the most likely diagnosis?
What is the most common site of acute aortic dissection?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app