
Vascular Pathology — MCQs

On this page
Histopathological examination of an elderly male patient reveals fragmentation of the elastic lamina, lymphocyte infiltration, and multinucleated giant cells. What is the most likely diagnosis?
In atherosclerosis, what leads to increased LDL in monocyte macrophages?
A 75-year-old woman presents with facial pain, headache, and intermittent visual symptoms. Temporal artery biopsies are performed. If the biopsies show abnormal vessels, which of the following would be the most likely pathological finding?
Which of the following are classified as small vessel vasculitis?
What type of arteritis may lead to myocardial infarction in children?
A mycotic aneurysm is an aneurysm infected because of-
Which of the following does not cause deep vein thrombosis?
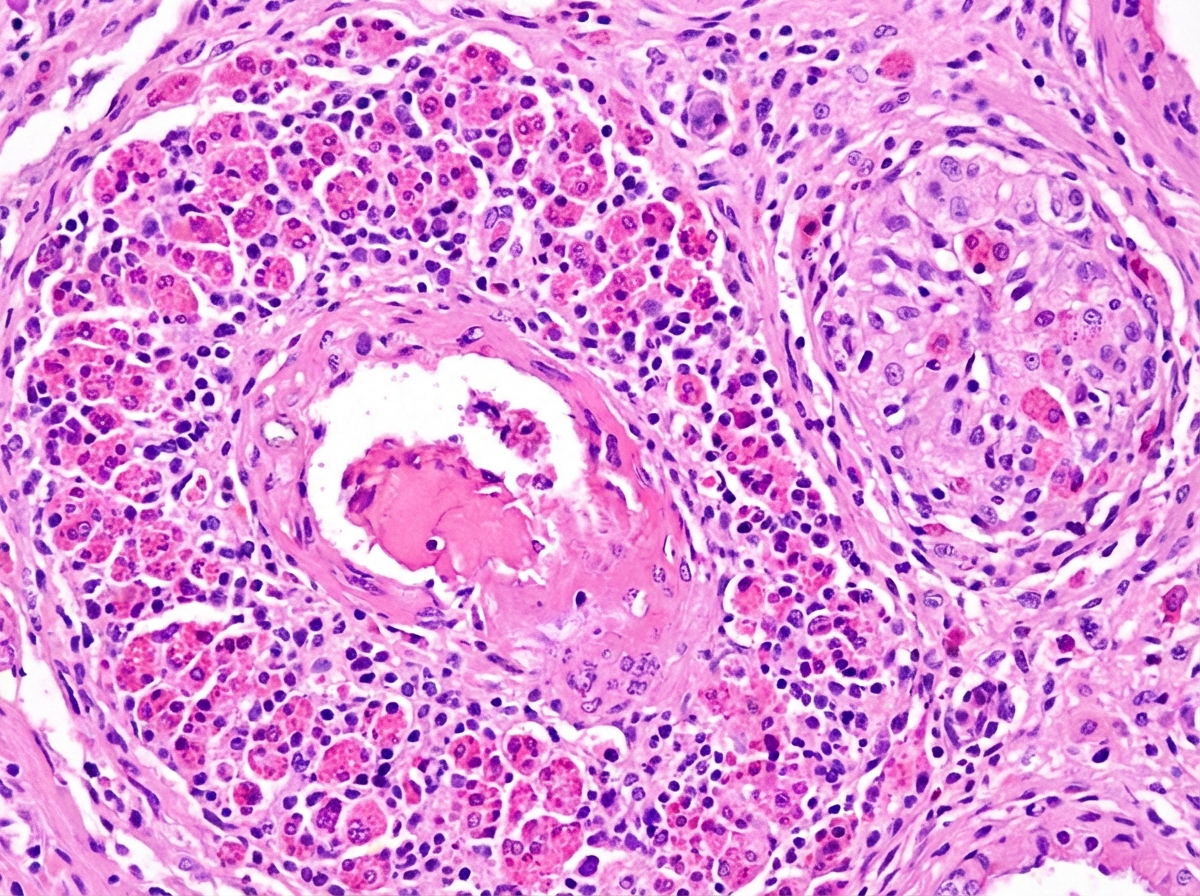
A 35-year-old patient presents with persistent allergic rhinitis, asthmatic episodes, and peripheral hypereosinophilia. Histological findings are shown below. What is your diagnosis?
The most commonly affected arteries seen by arteriography in Takayasu's arteritis is:
A 50-year-old hypertensive man develops very severe, "tearing" chest pain, which migrates from his upper back to mid-back over the period of an hour. Pathologic examination of a specimen removed from the patient during emergency surgery would MOST likely demonstrate which of the following?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app