
Vascular Pathology — MCQs

On this page
Which of the following vasculitis is NOT classified as a medium-vessel disease?
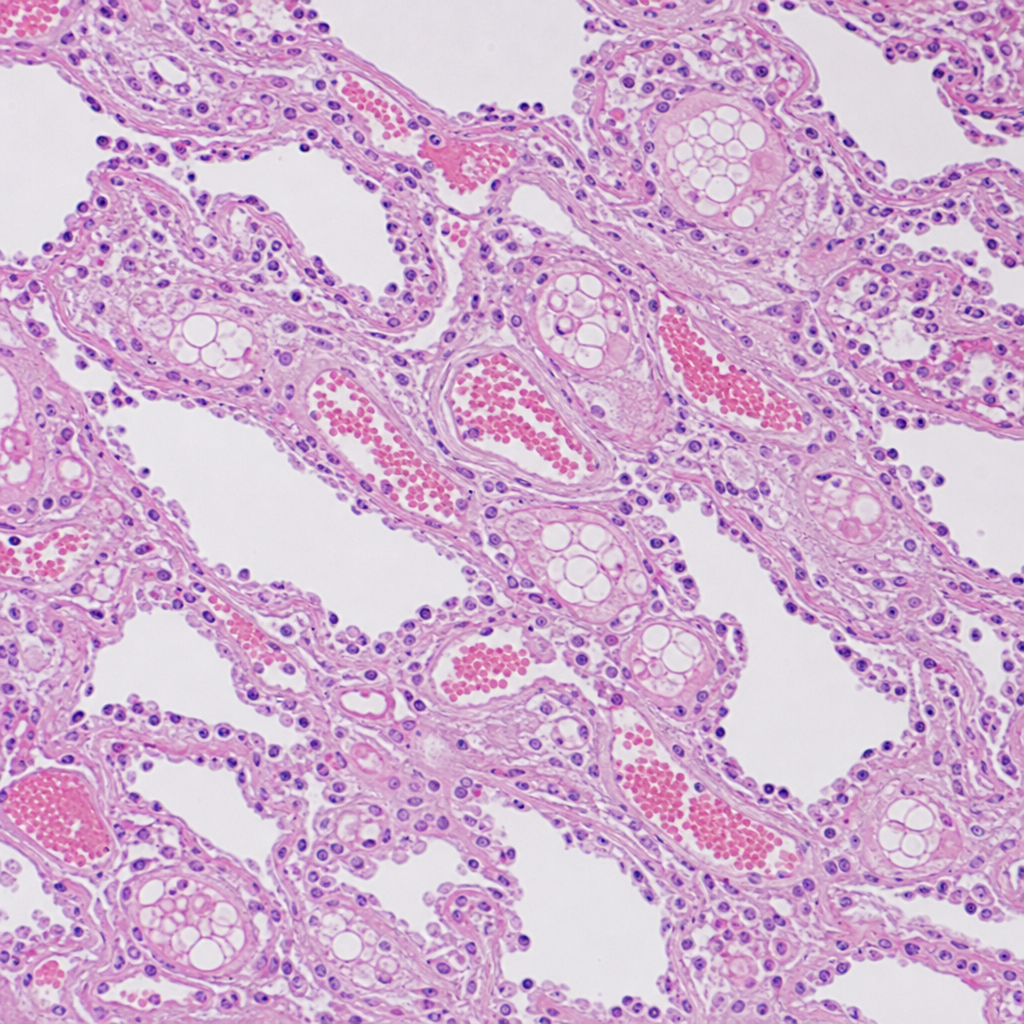
A 25-year-old male is brought to the emergency department 48 hours after sustaining a closed fracture of the right femur in a road traffic accident. He develops sudden onset confusion, petechial rash over the chest, and progressive hypoxia. Chest X-ray shows bilateral diffuse infiltrates. A lung biopsy specimen is stained with hematoxylin and eosin (H&E) on a paraffin section and examined (Image 1). Which of the following best explains the pathophysiological mechanism responsible for the pulmonary findings seen in this image?
Kaposi's sarcoma is a tumor of which system?
A 55-year-old woman presents with several weeks of fever, abdominal pain, weight loss, and fatigue. Three days prior to assessment, she developed a left foot drop. Her blood pressure is 160/90 mm Hg and pulse is 80/min. Physical examination confirms left peroneal nerve damage and a bilateral sensory neuropathy in both legs. There are no skin rashes. Laboratory evaluation reveals an ESR of 105 mm/h, WBC of 14,000/mL, and negative serologic tests for antineutrophil cytoplasmic antibody (ANCA) and ANA. The eosinophil count is normal, and urinalysis is negative for casts, protein, and red cells. A clinical diagnosis of polyarteritis nodosa is made. Which of the following is the most likely mechanism for renal injury in this condition?
Which multifocal tumor of vascular origin is commonly seen in patients with AIDS?
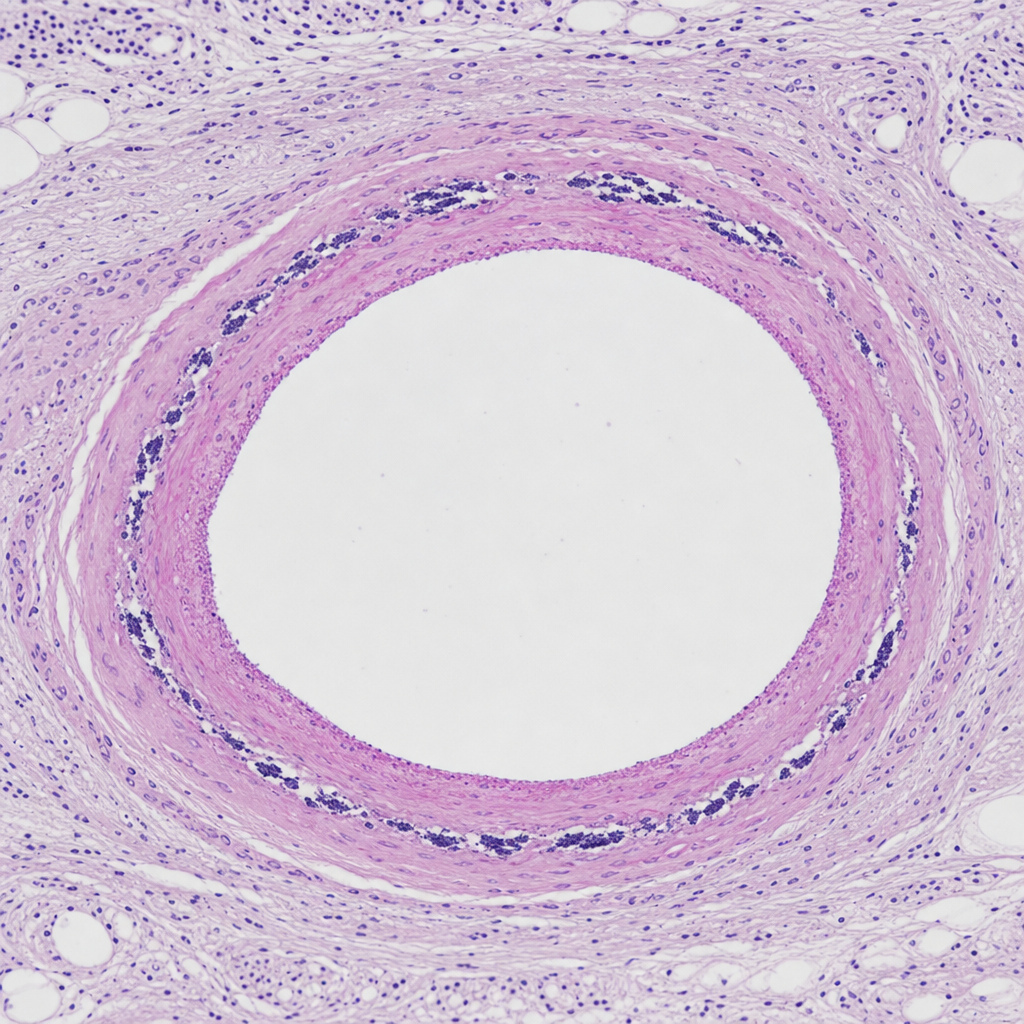
A 60-year-old asymptomatic female shows the following change in the tunica media of blood vessels. What is the diagnosis?
Which of the following diseases is more common in patients with alpha-1 antitrypsin deficiency?
A 60-year-old man has his left forearm amputated due to invasive rhabdomyosarcoma. The pathologist notes calcification in the wall of the radial artery, which otherwise appears unremarkable. Which of the following is the appropriate diagnosis?
Epithelioid hemangioendothelioma of the nose is classified as which of the following?
Which of the following conditions does NOT present with granulomatous vasculitis?
Practice by Chapter
Atherosclerosis
Practice Questions
Hypertensive Vascular Disease
Practice Questions
Aneurysms and Dissection
Practice Questions
Vasculitis
Practice Questions
Venous Disease and Thrombosis
Practice Questions
Vascular Tumors
Practice Questions
Varicose Veins and Lymphatics
Practice Questions
Pathology of Vascular Interventions
Practice Questions
Vascular Diseases in Specific Organs
Practice Questions
Congenital Vascular Anomalies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app