
Respiratory Pathology — MCQs

On this page
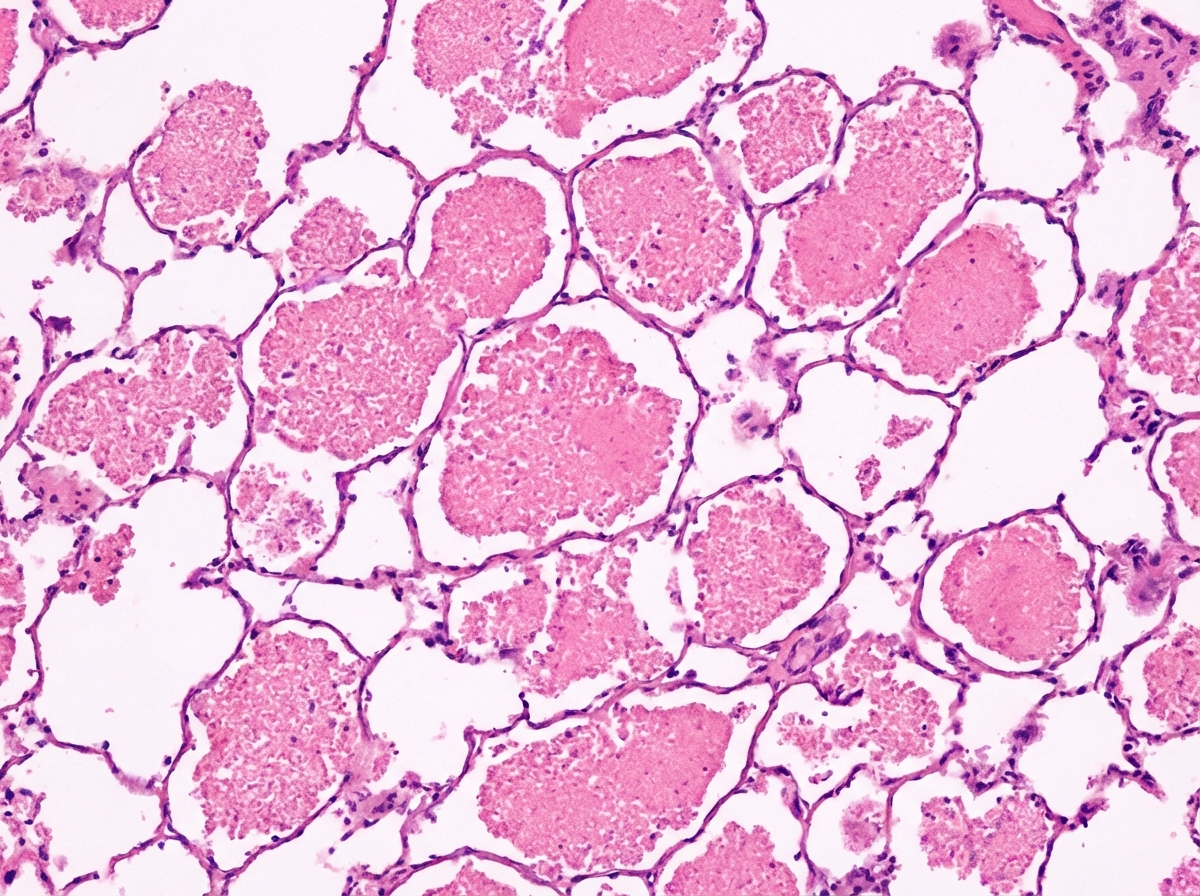
A full-term neonate develops severe progressive respiratory distress shortly after birth and subsequently dies. The image shows post-mortem lung biopsy findings. What is the most likely diagnosis?
Autopsy of a 23-year-old male victim of a motor vehicle accident reveals a small cluster of caseating granulomas in the right lung just above the interlobar fissure and similar granulomas in the hilar lymph nodes. Acid-fast staining demonstrates acid-fast bacilli within these lesions. No other lesions were found in the remaining organs and systems. Which of the following is the MOST accurate interpretation of these findings?
"Honeycomb lung" is most typical of which condition?
All of the following statements regarding centriacinar emphysema are true, except:
What is the most common clinical type of emphysema?
A 52-year-old woman has had a chronic cough for the past 2 years, accompanied by a small amount of occasionally blood-streaked, whitish sputum. On physical examination, her temperature is 37.9°C, pulse is 72/min, respirations are 22/min, and blood pressure is 125/80 mm Hg. Crackles are heard on auscultation over the upper lung fields. Heart sounds are faint, and there is a 15 mm Hg inspiratory decline in systolic arterial pressure. The chest radiograph shows prominent heart borders with a "water bottle" configuration. Pericardiocentesis yields 200 mL of bloody fluid. Infection with which of the following organisms is most likely to produce these findings?
Which of the following are true about alpha-1 antitrypsin deficiency?
Charcot laden crystals are found in which condition?
What is the most common termination of lobar pneumonia?
What is the primary complex of tuberculosis known as?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app