
Respiratory Pathology — MCQs

On this page
A 60-year-old man presents with chronic obstructive pulmonary disease (COPD). Which type of emphysema is most commonly associated with smoking?
A 55-year-old male with a history of chronic bronchitis is being evaluated for respiratory distress. Which pathophysiological process is primarily involved in chronic bronchitis?
A 65-year-old woman presents with progressive dyspnea and a productive cough. A CT scan reveals a lung mass and pleural effusion. A biopsy shows adenocarcinoma. Which of the following is a common histologic feature?
In RDS in a child, which cells are found defective?
Which of the following is a characteristic feature of chronic bronchitis?
Anthracosis is due to inhalation of?
Which type of pneumoconiosis is most commonly associated with tuberculosis (TB)?
Which of the following statements about silicosis is true?
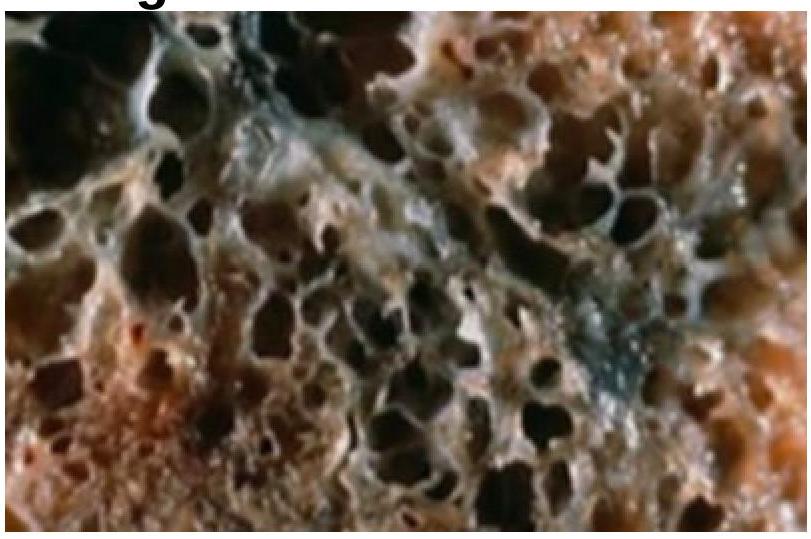
A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
Most common cause of idiopathic interstitial pneumonia is
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app