
Respiratory Pathology — MCQs

On this page
In which of the following forms of pulmonary carcinoma is the classic progression of metaplasia to dysplasia to carcinoma in situ observed?
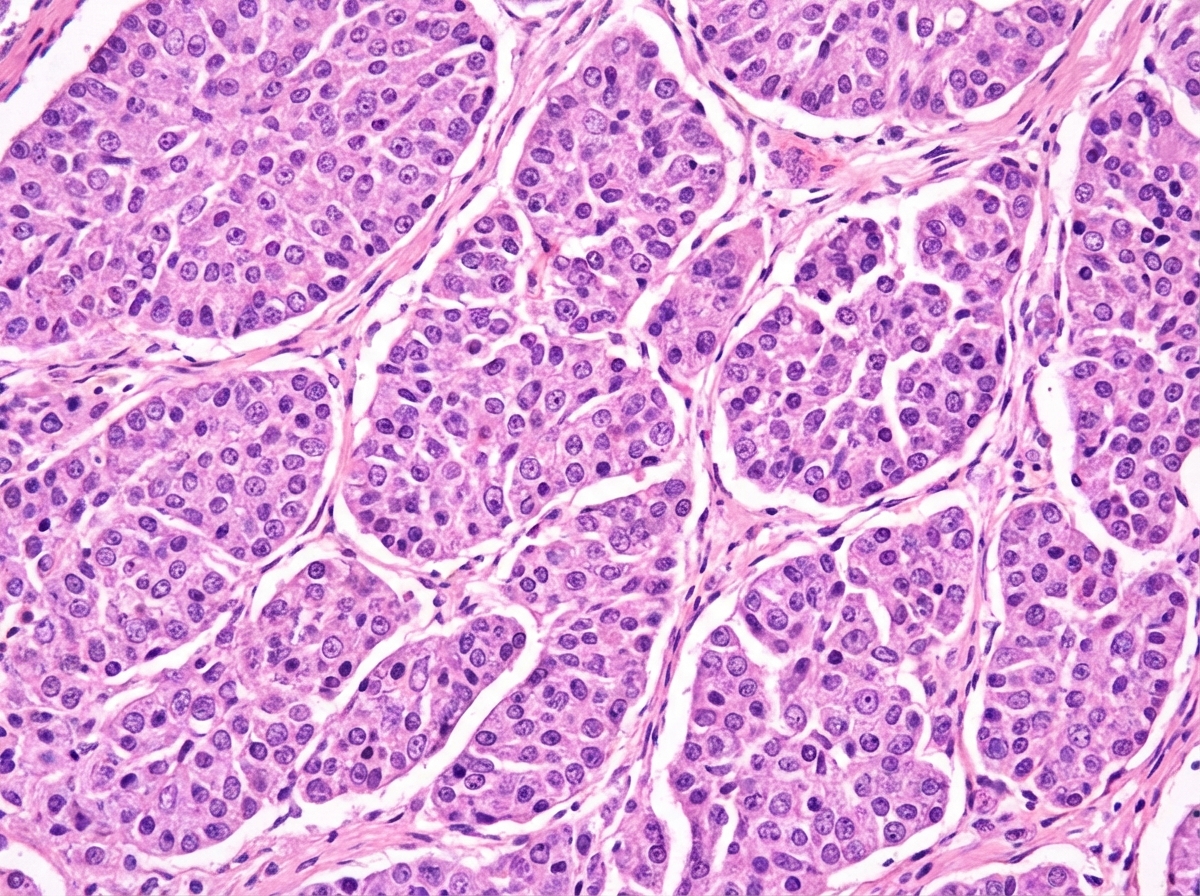
A 30-year-old woman presents with a history of fever for 2 weeks and multiple episodes of haemoptysis. Bronchoscopy shows a polypoid mass covered with intact mucosa. Surgical resection was performed, and the histology slide is shown below. What is the diagnosis?
Goodpasture's syndrome is characterized by?
A 60-year-old male with a long-standing history of breathlessness and heavy smoking since the age of 20 presents with an emaciated, anxious appearance and pursed-lip breathing, but without cyanosis. The chest is barrel-shaped. The primary pathology of the lung in this patient is associated with which of the following pathogenetic mechanisms?
Sudden death, right-sided heart failure (cor pulmonale or cardiovascular collapse) occurs when?
Cavitation of the lungs is not a feature of which of the following conditions?
Histologic sections of lung tissue from an individual with adult respiratory distress syndrome (ARDS) are most likely to reveal what finding?
A 45-year-old man is diagnosed with a nasopharyngeal tumor. Histologically, this neoplasm is composed of anaplastic cells immunoreactive for cytokeratin admixed with abundant lymphocytes. Which of the following factors is MOST likely implicated in the pathogenesis of this neoplasm?
A 56-year-old chronic smoker has a mass in the bronchus resected. What is the possible marker for this type of tumor?
Pleural fibroma is differentiated from mesothelioma by the presence of which of the following markers in the former?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app