
Respiratory Pathology — MCQs

On this page
An elderly male is known as a smoker presented with chronic cough, significant weight loss, and fatigue. Serum calcium level is raised. A lung biopsy was done, and it showed large atypical cells with hyperchromasia. What is the probable diagnosis?
What is the T stage classification for a lung carcinoma measuring 2.5 cm and not involving the pleura?
A 35-year-old woman with a long history of dyspnea, chronic cough, sputum production, and wheezing dies of respiratory failure following a bout of lobar pneumonia. She was not a smoker or an alcoholic. Which of the following underlying conditions is most likely associated with the pathologic changes shown in the lung autopsy?
In Respiratory Distress Syndrome (RDS) in a child, which type of cells are found to be defective?
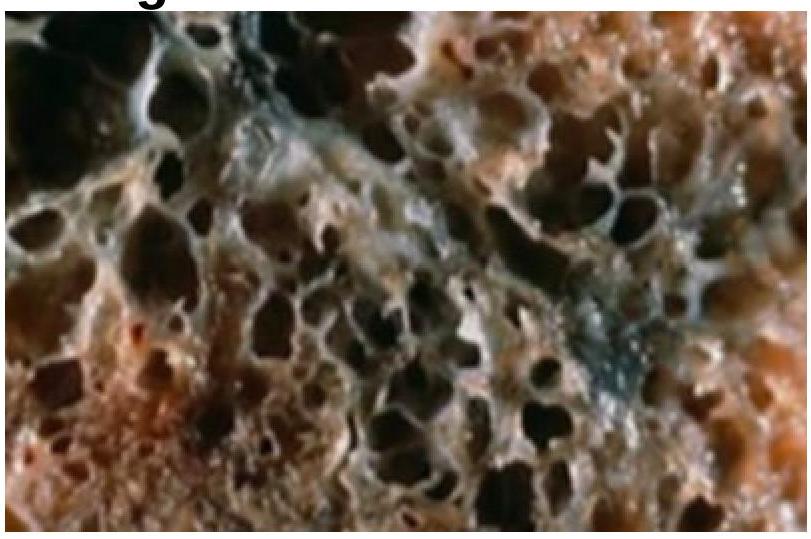
Identify the condition represented in the image.

Identify the condition shown in the image of a lung.

Most common cause of idiopathic interstitial pneumonia is
Radiotherapy induced radiation pneumonitis is mediated by all of the following cytokines and factors except -
Heart failure cells are seen in -
Which histological type of lung cancer is most commonly associated with metastasis?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app