
Respiratory Pathology — MCQs

On this page
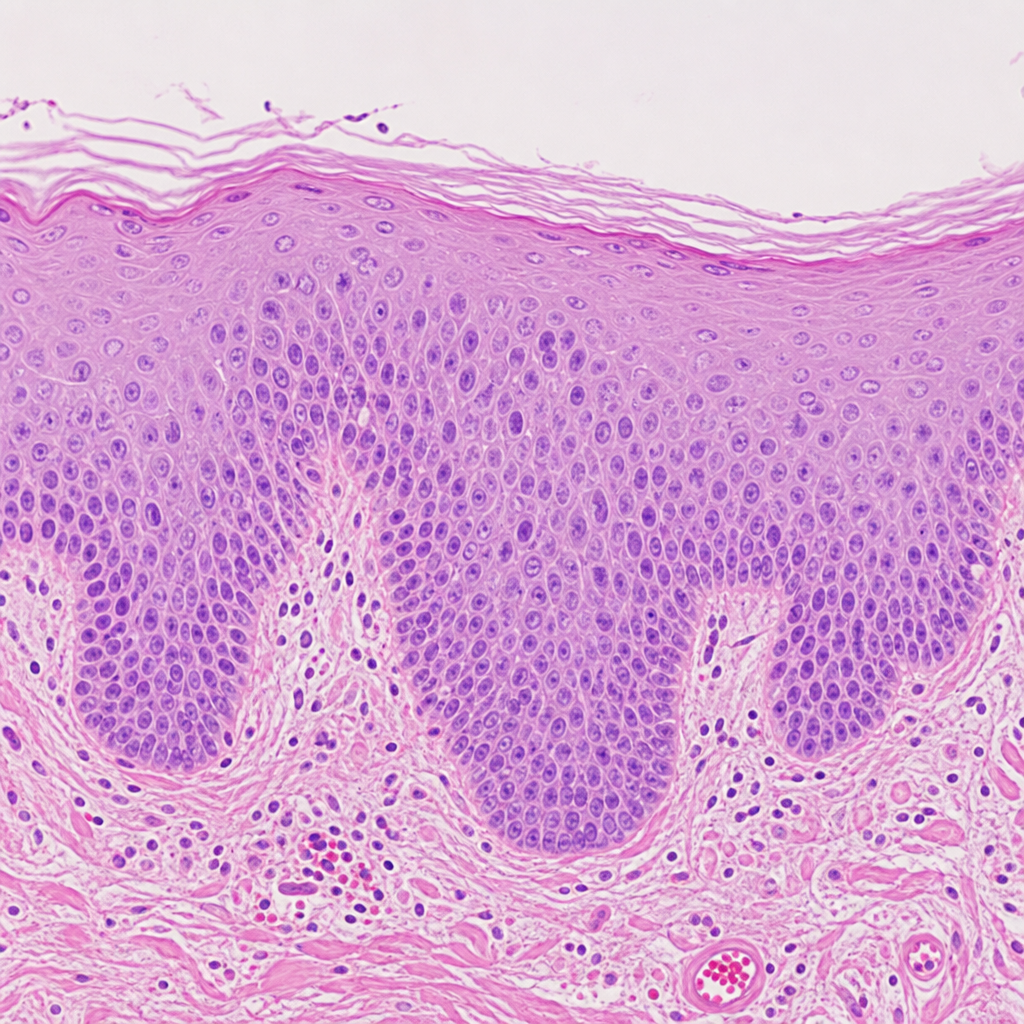
A 45-year-old man who is a chronic smoker came to the clinic with a complaint of cough. The physician examines the patient and takes a biopsy. The biopsy image is provided below. Which of the following cellular changes has happened to this patient?
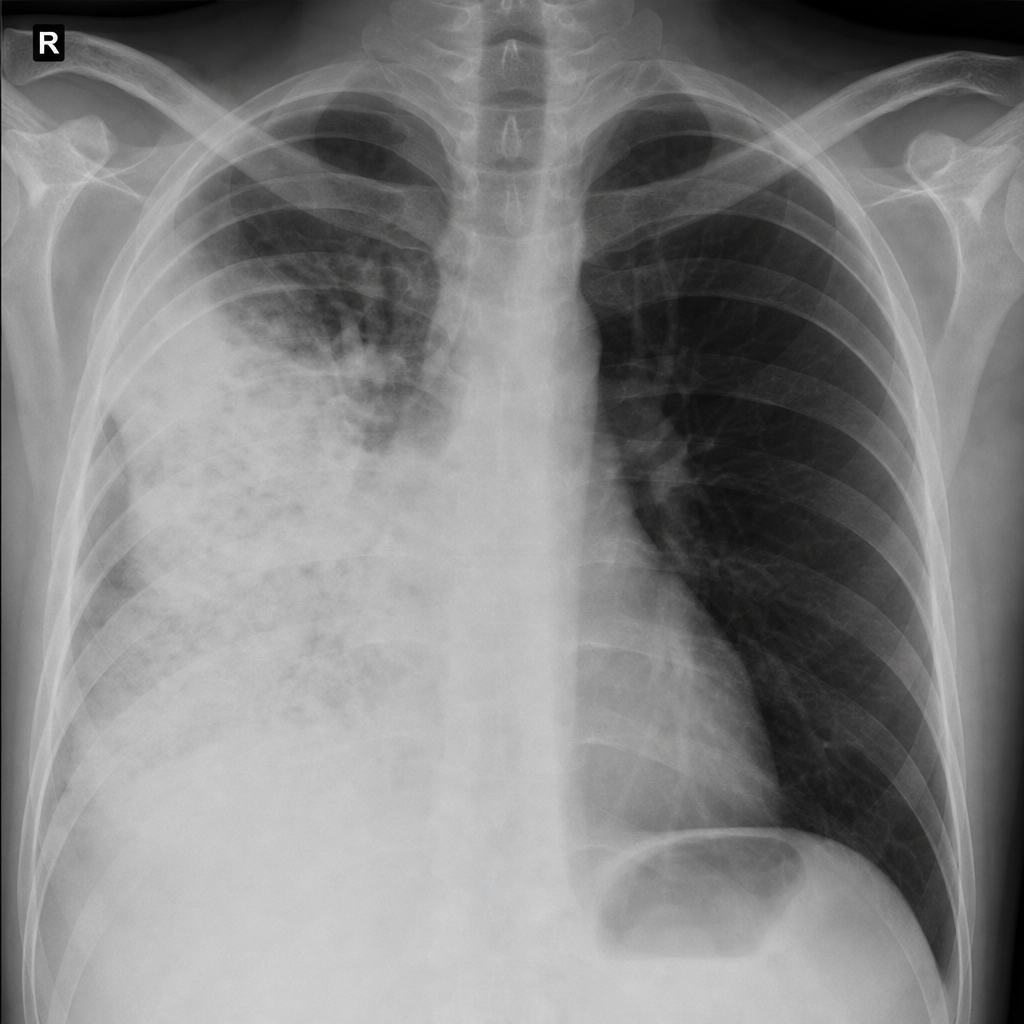
Identify the condition shown in the image of the lung.
Which of the following is a characteristic feature of chronic bronchitis?
Which of the following statements about silicosis is true?
In which type of lung carcinoma is the p53 mutation most commonly observed?
Which type of pneumoconiosis is most commonly associated with tuberculosis (TB)?
Granulomatous lung disease is caused by?
Metastasis to lungs comes most commonly from
Anthracosis is due to inhalation of?
In which condition is Calretinin primarily used as a diagnostic marker?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app