
Respiratory Pathology — MCQs

On this page
Which among the following has two general phases - first, simple pneumoconiosis and a second phase characterized by progressive massive fibrosis (PMF)?
A patient presents with respiratory distress and is diagnosed with panacinar emphysema. Which of the following is deficient?
A male patient is not responding to oxygen therapy and has been diagnosed with ARDS (Acute Respiratory Distress Syndrome). What is the role of IL-8 in ARDS?
TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
TTF-1 is a tumor marker for which of the following?
A male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
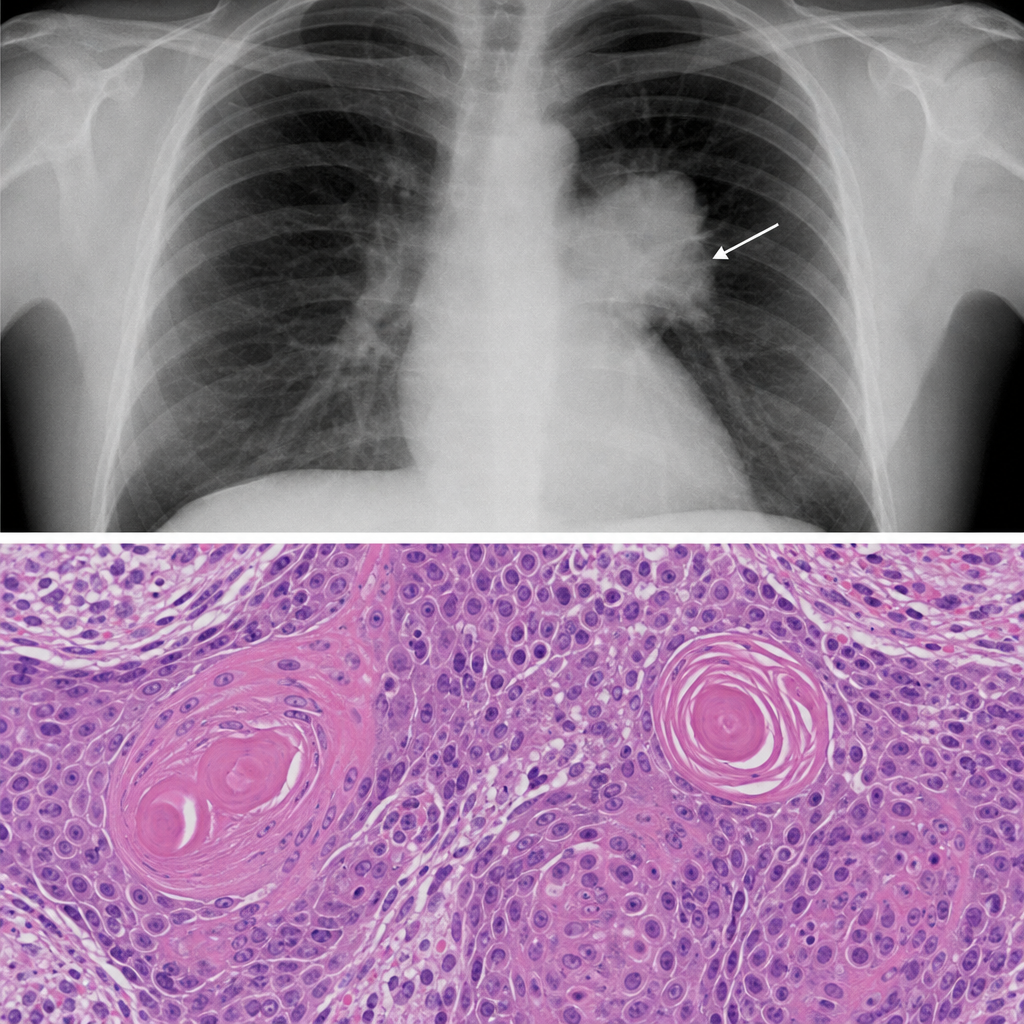
A male patient with hemoptysis. On examination, hilar mass was present. The histopathological image is shown below. Immunohistochemistry revealed that the cells were positive for p40. What is the diagnosis?
A 45-year-old man comes to the physician because of a productive cough and dyspnea. He has smoked one pack of cigarettes daily for 15 years. His temperature is 38.8°C (102°F). Physical examination shows decreased breath sounds and dullness on percussion above the right lower lobe. An x-ray of the chest shows a right lower lobe density and a small amount of fluid in the right pleural space. The patient's symptoms improve with antibiotic treatment, but he develops right-sided chest pain one week later. Pulmonary examination shows new scratchy, high-pitched breath sounds on auscultation of the right lobe. Histologic examination of a pleural biopsy specimen is most likely to show which of the following findings?
A CT scan shows the 'crazy paving' pattern in both lungs. Which bronchoalveolar lavage finding would confirm pulmonary alveolar proteinosis?
Heart failure cells are:-
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app