
Respiratory Pathology — MCQs

On this page
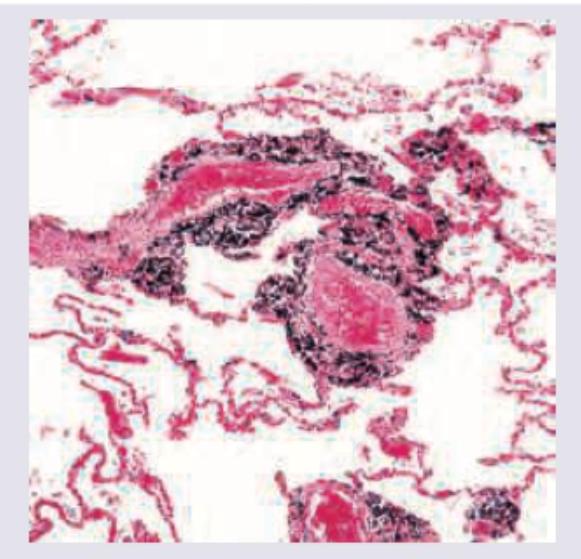
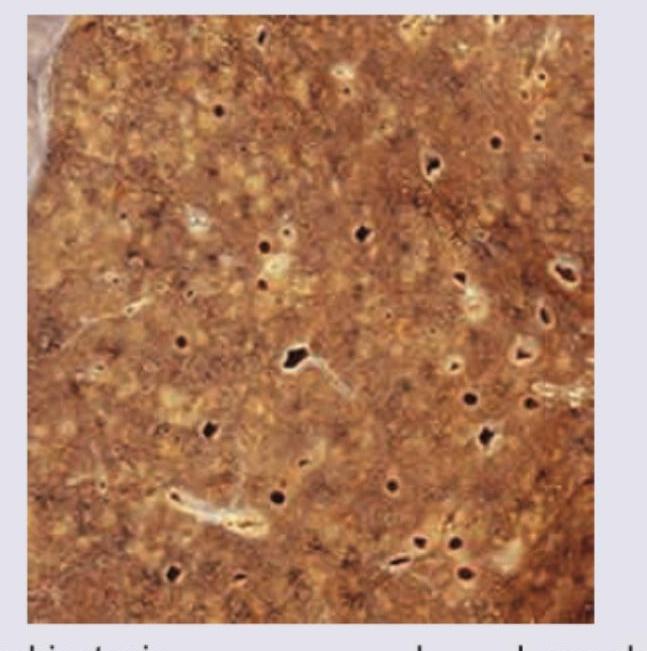
Lung biopsy of an urban city dweller shows presence of: (Recent NEET Pattern 2016-17)
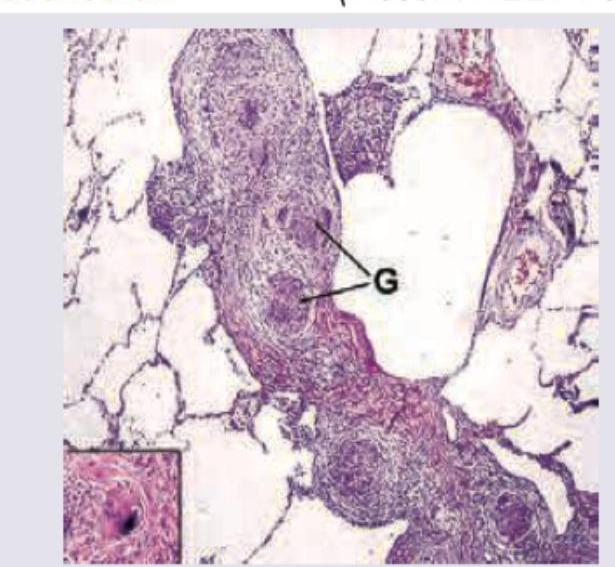
A 35-year-old female presents with difficulty in breathing at rest. On examination stridor is noted. The lung histopathological specimen shows presence of: (Recent NEET Pattern 2016-17)
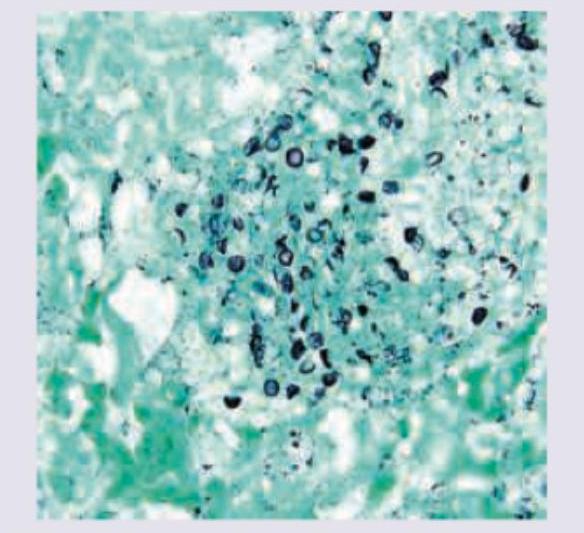
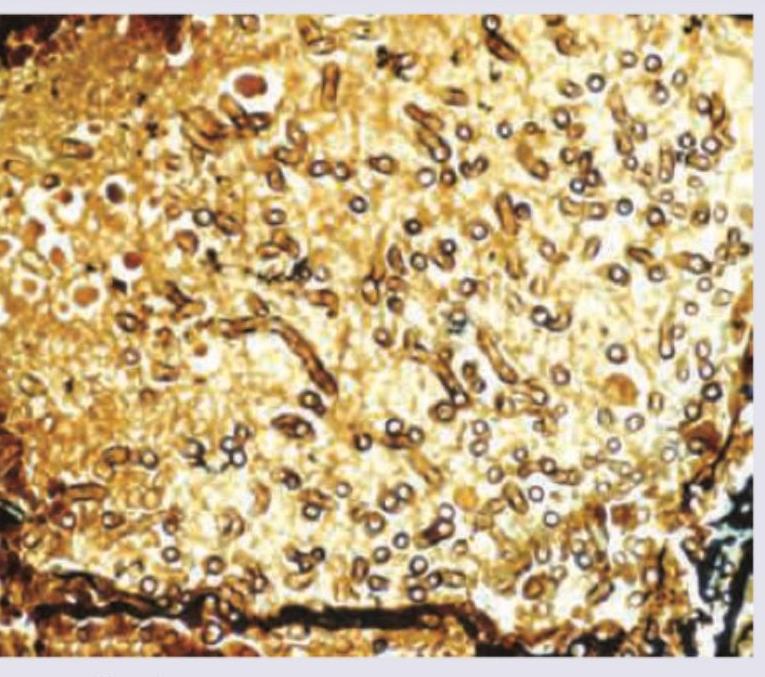
The following image of lung washing in AIDS positive patient is stained with:
A 25-year-old woman with ocular myasthenia Gravis on prednisolone for last 5 years is having cough with night sweats and significant weight loss. The lung histopathological specimen shows:
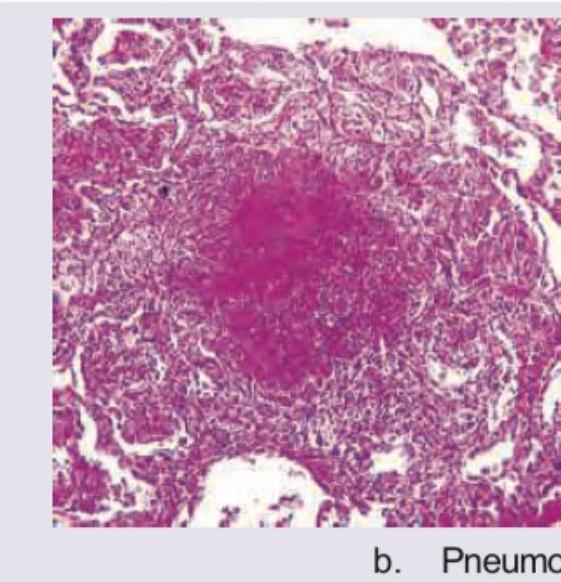
An 8-year-old boy with acute lymphoblastic leukemia on chemotherapy develops fever with nonproductive cough and respiratory distress. The lung specimen shows:
A 32-year-old chain-smoker presented with persistent productive cough, fever and recurrent pulmonary infections. After his death, lung specimen was extracted. Which of the components are destroyed?
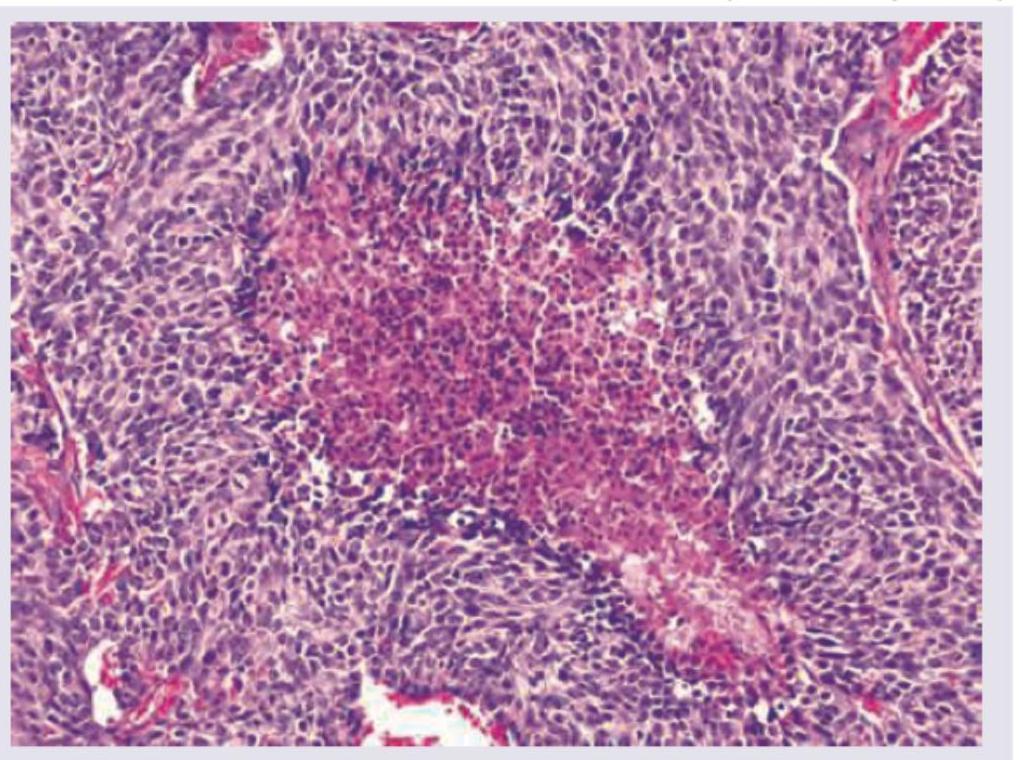
A 55-year-old male patient presented with a 4 month history of cough and hemoptysis. Bronchoscopy revealed an intrabronchial polyp. Biopsy from the polyp showed small cells with salt and pepper chromatin, with microscopic necrosis and 5 mitotic figures per 10 high power fields as shown below. Chromogranin staining was positive. What is the diagnosis and grade of the lesion based on the WHO pulmonary neuroendocrine tumor classification?
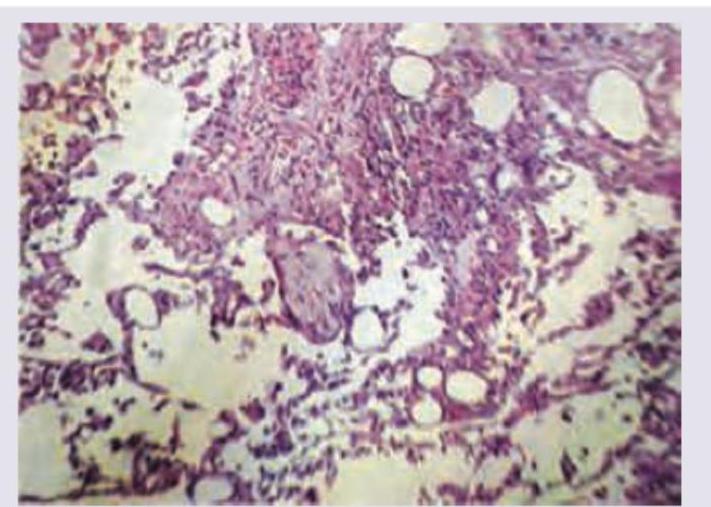
A patient with a depressive illness is brought to casualty with acute breathlessness. The patient was found unconscious at home and is known to have recently overdosed on sedative medication. X-ray shows diffuse infiltrates in right middle lobe and right lower lobe. The patient expired. The lung specimen on biopsy shows:
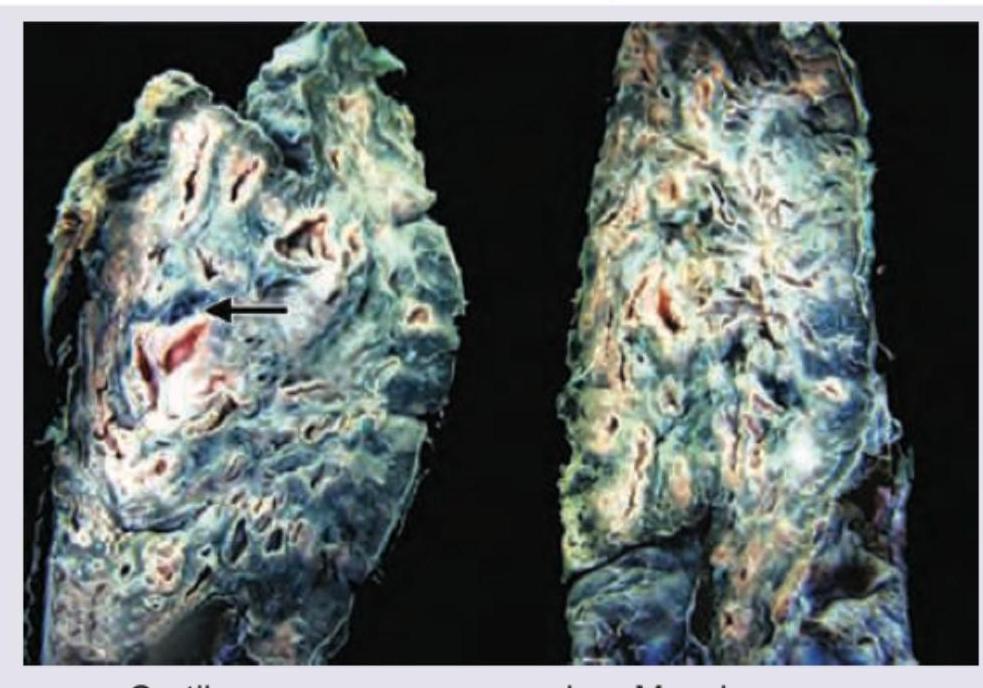
A 40-year-old man underwent lung transplantation. The resected lung specimen is shown below. Comment on the diagnosis.
'Masson Bodies' formed due to proliferation of immature collagen are a characteristic histopathological finding seen in which of the following conditions?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app