
Respiratory Pathology — MCQs

On this page
Lower lobe fibrosis is typically seen in which of the following conditions?
A 60-year-old person presents with a mass located at the central bronchus causing distal bronchiectasis and recurrent pneumonia. Which of the following findings is expected from a biopsy of the mass?
Lobar pneumonia is caused predominantly by which organism?
Which of the following types of bronchogenic carcinomas are most likely to develop within a residual area of peripheral scar tissue?
A 59-year-old male is found to have a 3.5-cm mass in the right upper lobe of his lung. A biopsy of this mass is diagnosed as a moderately differentiated squamous cell carcinoma. Workup reveals that no bone metastases are present, but laboratory examination reveals that the man's serum calcium levels are 11.5 mg/dL. This patient's paraneoplastic syndrome is most likely the result of ectopic production of which of the following?
Mediastinal lymph node calcification is seen in which one of the following conditions?
Asbestos exposure may be associated with which of the following malignancies?
Patient presents with dry cough, dyspnea and stridor. HPE of hilar LN shows stellate granulomas with giant cells and circular lamellated concretions on histopathology. Which of the following is the most likely diagnosis?
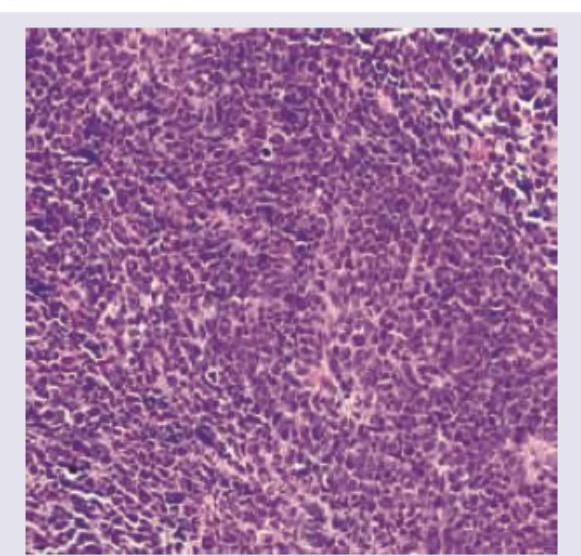
A 35-year-old patient presents with progressive cough and hemoptysis. Bronchoscopy shows 4 cm polypoidal mass projecting into bronchial lumen. CT guided lung biopsy image is given below. All are true about the condition shown except:
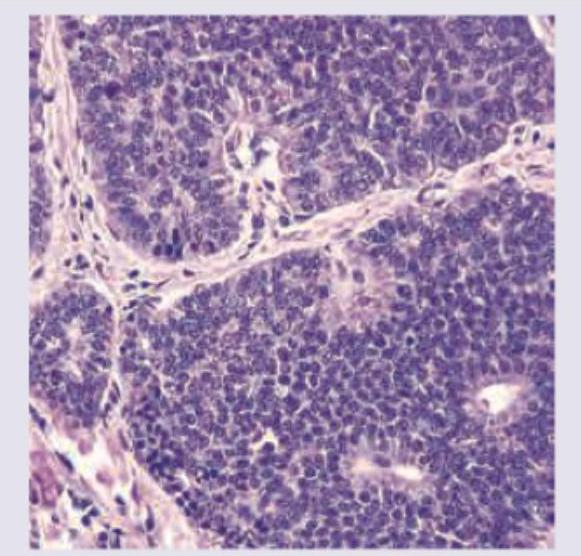
All are true about the type of lung cancer shown in the figure except: (Recent NEET Pattern 2016-17)
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app