
Respiratory Pathology — MCQs

On this page
Extensive pleural thickening and calcification, especially involving the diaphragmatic pleura, are classical features of which condition?
Intralobar sequestration of the lung is commonest in which segment?
A 65-year-old smoker presents with chronic cough, hemoptysis, and weight loss. Chest X-ray shows a cavitary lesion. What is the most likely diagnosis?
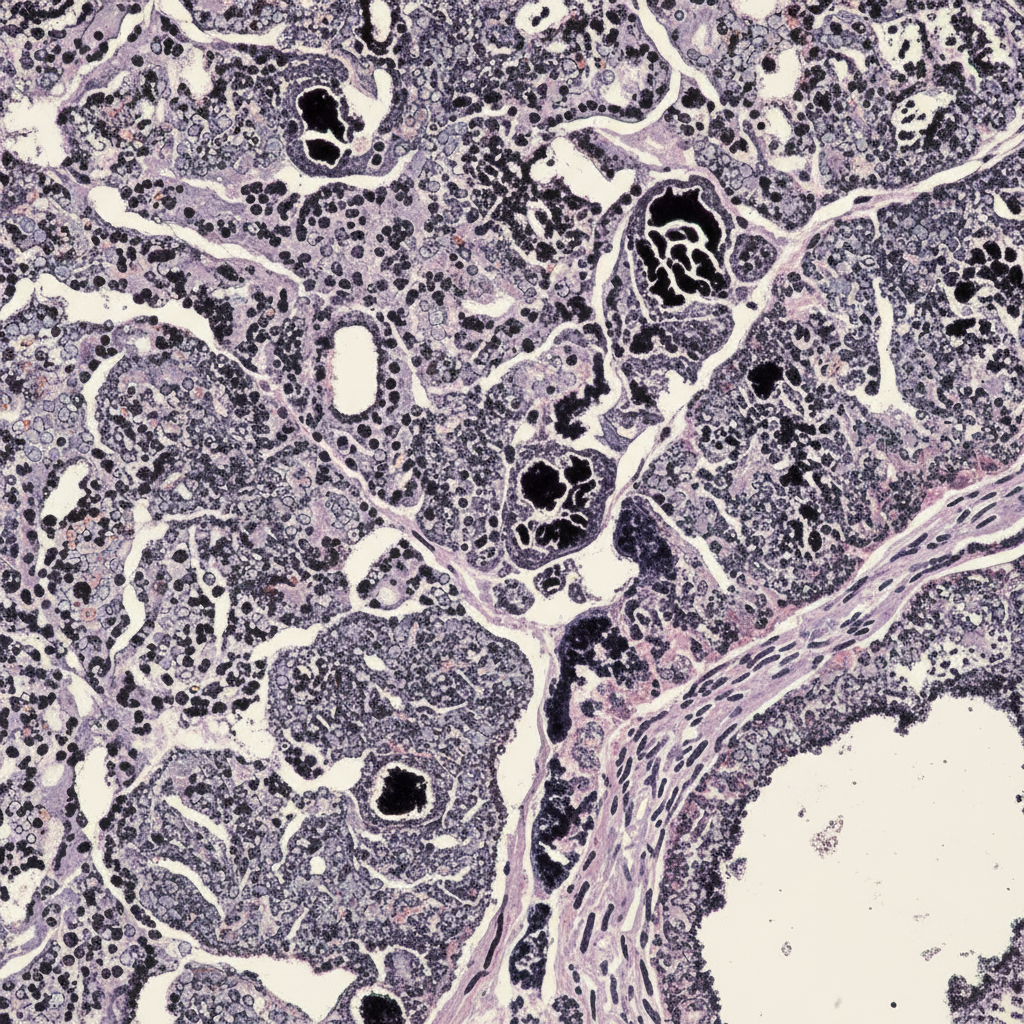
Examination of the lungs of a 55-year-old coal miner during autopsy reveals small hilar lymph nodes which are jet black in colour. The microscopic appearance of one lymph node is shown. What is the most likely diagnosis?
Periodic Acid Schiff (PAS) stain positive intra-alveolar material is seen in which of the following conditions?
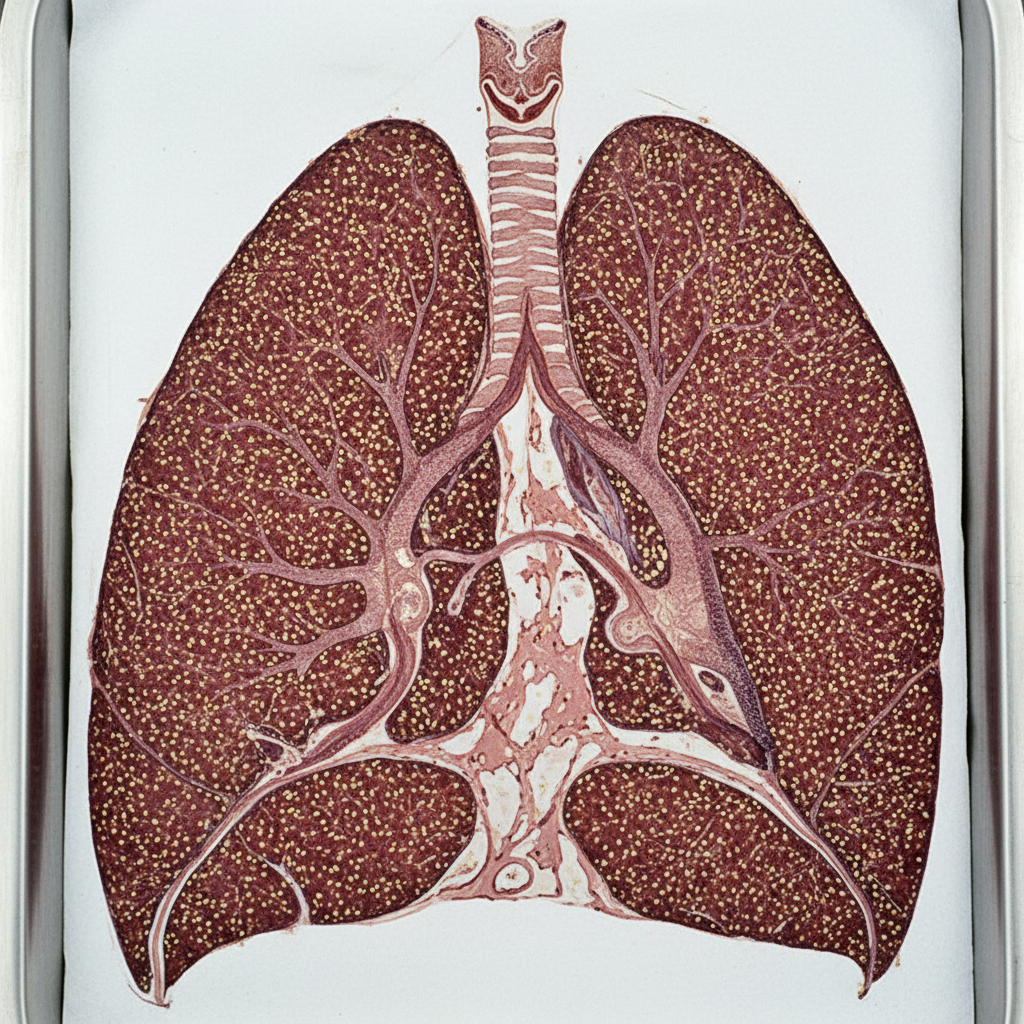
A patient underwent lung transplantation. Below is an anatomical illustration of the lung. What is the most likely diagnosis?
What is the characteristic feature of Kartagener's syndrome?
Asbestosis is associated with all of the following except:
Which condition is characterized by alveolar hemorrhage and hemosiderin-laden macrophages?
Which of the following is a finding in biopsy of mesothelioma of pleura?
Practice by Chapter
Congenital Anomalies
Practice Questions
Atelectasis and Acute Lung Injury
Practice Questions
Obstructive Pulmonary Diseases
Practice Questions
Restrictive Pulmonary Diseases
Practice Questions
Lung Infections
Practice Questions
Pulmonary Vascular Diseases
Practice Questions
Lung Tumors
Practice Questions
Pleural Diseases
Practice Questions
Interstitial Lung Diseases
Practice Questions
Occupational Lung Diseases
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app